Download
1 / 29
300 likes | 330 Vues
Learn about the background, pathophysiology, potential complications, presentation, bacteriology, principles of surgery, and considerations in revascularization and endovascular surgery for this complex condition.

E N D
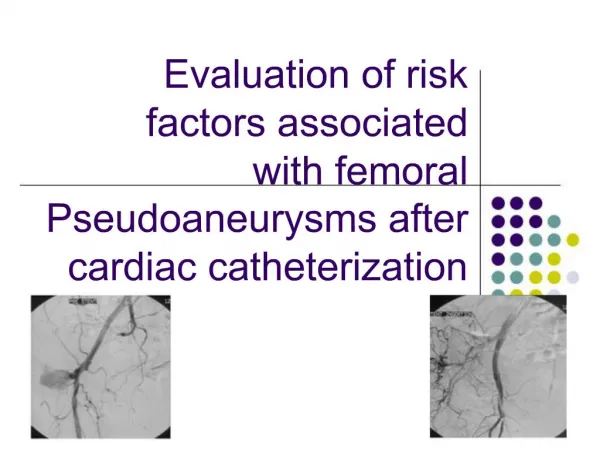
Ruptured Infected Femoral Artery Pseudoaneurysms in IV Drug Addicts Winston Wong, Yan Chai Hospital JHSGR July 18 2015
Next 10 minutes… • Background • Management • Controversies
Background • IV drug abuse is an increasing problem with concomitant increase in its complications • Vascular complications from IV drug abuse is on the rise • Infectious pseudoaneurysms • Deep vein thrombosis • Venous gangrene • Arterial embolization • Infected pseudoaneurysms of the femoral artery are one of the most common arterial complications in IV drug abusers
Pathophysiology • Repeated non-sterile punctures aimed at finding easy peripheral venous access • Extravasation of blood • Contamination of the subsequent hematoma • Erosion and eventual rupture of the vessel wall • Formation of infected pseudoaneurysm
Potential complications • Distal embolization • Limb loss • Sepsis • Rupture with rapid blood loss • Death
Presentation • Groin injection site • Groin mass • Drainage / bleeding • Pulsatility • Thrill • Absent pedal pulses • Inability to extend hip • Septicemia
Overview • Background • Management • Controversies
Broad spectrum IV antibiotics Universal contact precaution Adopted from Tan et al, World J Surg. 2009
Bacteriology? • Pre-antibiotic era: Enterococcus, streptococcus [1] • Post-antibiotic era: Staph aureus, Salmonella [1] • Ting & Cheng (HK)[2] MSSA • Jayaramans (US)[3], Saini (India)[4]Staph aureus (majority), Pseudomonas, E coli • Brossier et al (France)[5] Majority from atypical bacteria e.g. Campylobacter, Listeria, MTB, CoxiellaStaph aureus (4%)
Principles of surgery • Stop bleeding • Debride infective tissue • Preserve distal circulation • Conservative management is rarely an option
Overview • Background • Management • Controversies
Proposed treatments? [6] • Ligation & excision (Lig-Exc) alone • Lig-Exc + immediate revascularization • Lig-Exc + delayed revascularization + Debridement of infective tissue
Ligation & excision • Single vs triple ligation (CFA, SFA, PFA) • Benefits • Faster, more straightforward • Require less resources & expertise • Complications • Claudication (~40-50%, some studies up to 100% [7]) • Amputation (none to 35.0% [6])
Ligation & excision • Cheng et al, 1992 [8] • 21 infected femoral pseudoaneurysms • 19 ligations only, 2 with revascularization • 14 reported claudication (74% of ligation only) • Ting & Cheng, 1997 [2] • 33 infected femoral pseudoaneurysms • 24 triple ligation, 10 single ligation • 4 asymptomatic and rest had some degree of claudication • No limb loss in both studies
Considerations in revascularization? • Revascularization is challenging and often require special technical considerations • Autogenous vs synthetic grafts? • Autogenous veins are more resistant to infection, but not always available [6] • Arterial grafts (e.g. internal iliac artery) [9] • Synthetic grafts [6,10] • Significantly higher risk of reinfection • Life-threatening hemorrhage if used as route for injections
Considerations in revascularization? • Extra-anatomic vs in-situ bypass? • In-situ bypass through infected field is controversial • Extra-anatomic via lateral thigh or obturator route • High chance of graft failure requiring removal • Immediate vs delayed revascularization? • Close observation for signs of limb ischemia • Worse outcome if delay in revascularization > 6 hrs [11] • Contraindications? • Presence of extensive tissue necrosis • Necrotizing fasciitis
Endovascular surgery? • Emerging interest as scattered reports of successful repair of infected aneurysms in several territories • Minimally invasive alternative / bridge to open surgery • Prosthesis in infected field is always debatable
Endovascular surgery? • Handful of case reports only for endovascular intervention for ruptured femoral infected pseudoaneurysms [15, 16] • ? Prolonged / lifelong suppressive antibiotic regimen • 6 weeks? 6 months? Lifelong? • ? Antiplatelets / anticoagulation • ? Long-term consequences • ? Patient selection
In the middle of the night… • Resuscitation • Surgery • Hemostasis - ligate involved arteries • Infection control - excise pseudoaneurysm, debride tissue • Bacteriology – save pus / wall for cultures • Wound – leave open / partial close for dressing • Beware of needle prick! • Post-op • +/- Revascularization
Conclusion • The best surgical management of infected femoral pseudoanerysms remain controversial • Simple ligation & excision with debridement is the most common approach, with considerable risk of severe claudication, critical ischemia, and amputations in some individuals • Revascularization aim to avoid gangrene, maintain limb viability, and lower claudication rates, but need to accept the major risk of significant and life-threatening secondary complications
[1] Hussain MA, Roche-Nagle G. Infected pseudoaneurysm of the superficial femoral artery in a patient with Salmonella enteritidis bacteremia. Can J Infect Dis Med Microbiol. 2013;24(1):e24-e25 [2] Ting AC, Cheng SW. Femoral pseudoaneurysms in drug addicts. World J Surg. 1997;21(8):783-6 [3] Jayaramans et al. Mycotic pseudoaneurysms due to injection drug use: a ten-year experience. Ann Vasc Surg. 2012;26(6):819-24 [4] Saini et al. Infected pseudoaneurysms in IV drug abusers: ligation or reconstruction? Int J Appl Basic Med Res 2014;4:S23-26 [5] Brossier et al. New bacteriological patterns in primary infected aorto-iliac aneurysms: A single-centre experience. Eur. J. Vasc. Endovasc. Surg 2010;240;582-88 [6] Georgiadis GS et al. Surgical treatment of femoral artery infected false aneurysms in drug abusers. ANZ J. Surg. 2005; 75: 1005-1010 [7] Gan et al. Outcome after ligation of infected false femoral aneurysms in intravenous drug abusers. Eur. J. Vasc. Endovasc. Surg. 2000; 19:158-61 [8] Cheng SWK et al. Infected femoral pseudoaneurysm in intravenous drug abusers. Br. J. Surg. 1992; 79:510-12. [9] Tsao JW et al. Presentation, diagnosis and management of arterial mycotic pseudoaneurysms in injection drug users. Ann. Vasc. Surg. 2002; 16: 652-62 [10] Reddy DJ et al. Infected femoral artery false aneurysms in drug addicts: Evolution of selective vascular reconstruction. J. Vasc. Surg. 1986; 3: 718-24 [11] Benitez PR, Newell MA. Vascular trauma in drug abuse: patterns of injury. Ann Vasc Surg 1986; 1:175–181 [12] Arora S et al. Common femoral artery ligation and local debridement: a safe treatment for infected femoral artery pseudoaneurysms. J. Vasc. Surg. 2001; 33: 990-3 [13] Tan KK et al. Surgical management of infected pseudoaneurysms in intravenous drug abusers: single institution experience and a proposed algorithm. World J Surg. 2009 Sep;33(9):1830-5 [14] Yegane RA et al. Surgical Approach to Vascular Complications of Intravenous Drug Abuse. European Journal of Vascular and Endovascular Surgery 2006; 32(4):397-401 [15] Klonaris et al. Emergency stenting of a ruptured infected anastomotic femoral pseudoaneurysm. Cardiovasc Intervent Radiol 2007;30:1238-41 [16] Psathas et al. Management of a complicated ruptured infected pseudoaneurysm of the femoral artery in a drug addict. Case Reports in Vascular Medicine 2012; Article ID 434768 References
Q & A Ruptured Infected Femoral Artery Pseudoaneurysms in IV Drug Addicts
Investigation? • Active bleeding Urgent surgery • CT angiography • Duplex USG • Angiography • MR angiography
Limitations of current studies • High proportion of patients lost to follow-up • No study ever achieved complete post-surgery follow-up except in acutely symptomatic drug addicts • No fixed protocol for surgical management • Based on surgeon preferences • Mostly small scale, retrospective studies
YCH • 3 cases in past 6 months (Jan – June 2015) • 2 ligation + excision • 1 DAMA on POD1 • 1 discharged on POD3 • 1 death (hemorrhagic shock)
Prediction of need for revascularization? • No reliable subjective measures • Non-palpable pulses • Systolic pressure in PFA <40 mmHg (Padberg et al, 1992) • Lack of pedal Doppler scan signal after ligation or at test clamping of EIA (Arora et al 2001) • When patient is alert • Clinical assessment by pain in foot and calf, decreased power & range • Absence of pulse / positive Doppler signal does not necessitate immediate amputation
ABI • Normal 1.0 – 1.4 • <0.9 = PAD • >1.4 calcification / vessel hardening • 0.9-1 – acceptable • 0.8-0.9 – some arterial disease • 0.5-0.8 – moderate disease • <0.5 – severe disease