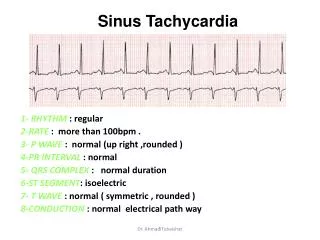
Wide Complex Tachycardia
Jay Green Emergency Medicine Resident, PGY-3 July 24, 2008. Wide Complex Tachycardia. Objectives. Improve our ability to distinguish various WCT. Regular WCT VT (monomorphic) SVT + accessory pathway SVT + BBB SVT with a Na channel blocker. Irregular WCT Polymorphic VT

Wide Complex Tachycardia
E N D
Presentation Transcript
Jay Green Emergency Medicine Resident, PGY-3 July 24, 2008 Wide Complex Tachycardia
Objectives Improve our ability to distinguish various WCT Regular WCT • VT (monomorphic) • SVT + accessory pathway • SVT + BBB • SVT with a Na channel blocker Irregular WCT • Polymorphic VT • Torsades de Pointes • A fib + accessory pathway • A fib + BBB • A flutter + variable block + BBB • MAT + BBB • V Fib
An Approach to WCT • (Is the patient stable or unstable?) • What is the rate? • Is the rhythm regular or irregular? • Are there p waves? • Are they related to the QRS? • Are they flutter waves? • Are the p waves of the same morphology? • Is the QRS morphology consistent?
35M palpitations, lightheaded Irregular WCT, marked variation in QRS morphology, no P waves = AF + WPW
Wolff-Parkinson-White Syndrome • Most common ventricular pre-excitation syndrome (bundle of Kent) • Triad: • Short PR (<0.12 sec) • QRS prolongation (>0.10 sec) • Slurred QRS upstroke (delta wave) • If WCT • Rates can approach 300bpm • Significant QRS morphology variation
57M weakness, palpitations Irregular WCT, consistent QRS morphology, no P waves = AF + RBBB
44M chronic alcoholic, unresponsive Irregular WCT, varying QRS morphology (undulating) = Torsades de Pointes
47M palpitations Irregular WCT, consistent QRS morphology, P waves, consistent R-R in groups = A flutter + variable block + RBBB
60M dyspnea, palpitations, hx COPD Irregular WCT, consistent QRS morphology, irregular P waves, inconsistent R-R = MAT + RBBB
Summary Irregular WCT – The Bad • AF + WPW • QRS morphology variation • Rates can approach 300bpm • AF + BBB • Consistent QRS morphology • Rate limited by AV node (usually < 200bpm) • Polymorphic VT • QRS morphology variation (more chaotic than WPW) • Rates consistently rapid (often > 300bpm) • Unstable
Summary Irregular WCT – The Good • Atrial flutter with variable block + BBB • P waves present, some not conducted • Consistent QRS morphology • Consistent R-R interval in groups • MAT + BBB • Irregular P waves of different morphology • Consistent QRS morphology • Inconsistent R-R interval
41M weakness Irregular wide complex rhythm, peaked T, no P = hyperkalemia
ECG Findings in Hyperkalemia • Peaked T-waves (>5mm) • QT shortening • ST elevation • Increased PR/loss of P wave • Widening/Slurring QRS • Sine wave appearance • Potentially mistaken for VT • 2nd/3rd degree block, VF, asystole
72F SOB, PMH: recent MI Regular WCT, AV dissociation & fusion beat (rhythm strip), capture beat (V1) = VT
61M fever, cough, dyspnea Regular WCT, P waves in V1 = atrial tachycardia + LBBB
VT vs. SVT With Abberancy • Angina, MI, CABG, valvular dz, or CHF PPV 95% for VT • Hemodynamic stability not useful • ECG findings • A-V dissociation (discernable in 20%) • PPV 100% • AV association not helpful (present in 50% VT) • Fusion beats, capture beats (discernable in 5-10%) • PPV 100%
VT vs. SVT With Abberancy • Wellens criteria • Many criteria • Wellens HJJ, Bar FWHM, Lie KI. The value of the electrocardiogram in the differential diagnosis of a tachycardia with a widened QRS complex. Am J Med 1978;64:27-33. • Brugada criteria • 4-step approach using Wellens • SN 98.7%, SP 96.5% for VT (original study) • Brugada P: A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex, Circulation 83:1649, 1991. • EP’s: SN 79-83%, SP 43-70%, K = 0.54-058 • Isenhour et al. Wide Complex tachycardia: continued evaluation of diagnostic criteria. Academic Emergency Medicine. Jul 2000;7(7): 769-773. • Herbert et al. Failure to agree on the electrocardiographic diagnosis of ventricular tachycardia. Ann Emerg Med. 1996;27(1):35-8.
Summary Regular WCT • VT • Fusion beats, capture beats, AV dissociation • PMH: cardiac disease • SVT + BBB • Absence of fusion/capture beats and AV dissociation • Pre-existing BBB • SVT + accessory pathway • Absence of fusion/capture beats and AV dissociation • Pre-existing accessory pathway • SVT + Na channel blocker
64F SOB, hypotension, PMH: a fib Regular WCT, bidirectional = Digoxin toxicity
60 M with CP and hypotension Irregular WCT, rate > 250, inconsistent QRS morphology = AF + WPW
62F palpitations Irregular WCT, consistent QRS morphology = AF + RBBB
63F syncope, PMH: DM & arthritis Hyperkalemia
43M severe palpitations Regular WCT, no P waves = presumed VT What if old ECG with pre-existing RBBB? = SVT
62F lightheaded, PMH: MI x 2 Regular WCT, no P waves = VT
61M palpitations, lightheaded Regular WCT, AV dissociation in V1 & II = VT
74M CP, palpitations Rhythm strip Fusion beat Regular WCT, no P waves, fusion beat = VT