Download
1 / 61
610 likes | 705 Vues
Learn about acute pancreatitis, its causes, symptoms, evaluation, and radiographic imaging. Dive into prognosis, scoring systems, and therapeutic strategies. Knowledge to help combat this condition effectively.

E N D
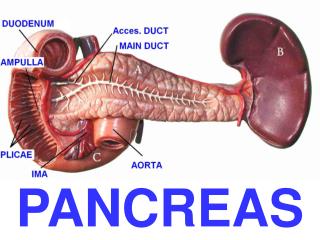
Pancreas Inflammation & cancer By AMGAD FOUAD Professor Of Surgery Gastroenterology Center Mansoura University.
Acute pancreatitis Pathophys- insult leads to leakage of pancreatic enzymes into pancreatic and peripancreatic tissue leading to acute inflammatory reaction
Acute pancreatitis • Etiologies • Idiopathic • Gallstones (or other obstructive lesions) • EtOH • Trauma • Steroids • Mumps (& other viruses: CMV, EBV) • Autoimmune (SLE, polyarteritisnodosa) • Scorpion sting • Hyper Ca, TG • ERCP (5-10% of pts undergoing procedure) • Drugs (thiazides, sulfonamides, ACE-I, NSAIDS, azathioprine) EtOH and gallstones account for 60-70% of cases
“Less Common” causes • Pancreas divisum • Chinese liver fluke • Ischemia (bypass surgery) • Cystic fibrosis
Trivia • What is the name of the scorpion that causes pancreatitis? • Hint: you won’t find it in the USA • ) • TityusTrinitatis (Found in Central) • South America and the Caribbean
Signs & Symptoms • Severe epigastric abdominal pain - abrupt onset (may radiate to back) • Nausea & Vomiting • Weakness • Tachycardia • +/- Fever; +/- Hypotension or shock • Grey Turner sign - flank discoloration due to retroperitoneal bleed in pt. with pancreatic necrosis (rare) • Cullen’s sign - periumbilical discoloration (rare)
Grey Turner sign Cullen’s sign
Differential • Not all inclusive, but may include: • Biliary disease • Intestinal obstruction • Mesenteric Ischemia • MI (inferior) • AAA • Distal aortic dissection • PUD
Evaluation • amylase…Nonspecific !!! • Amylase levels > 3x normal very suggestive of pancreatitis • May be normal in chronic pancreatitis!!! • Enzyme level severity • False (-): acute on chronic (EtOH); HyperTG • False (+): renal failure, other abdominal or salivary gland process, acidemia • lipase • More sensitive & specific than amylase
Evaluation • Other inflammatory markers will be elevated • CRP, IL-6, IL-8 (studies hoping to use these markers to aid in detecting severity of disease) • ALT > 3x normal gallstone pancreatitis • (96% specific, but only 48% sensitive) • Depending on severity may see: • Ca • WBC • BUN • Hct • glucose
Radiographic Evaluation • AXR - “sentinel loop” or small bowel ileus • US or CT may show enlarged pancreas with stranding, abscess, fluid collections, hemorrhage, necrosis or pseudocyst • MRI/MRCP newest “fad” • Decreased nephrotoxicity from gadolinium • Better visualization of fluid collections • MRCP allows visualization of bile ducts for stones • Does not allow stone extraction or stent insertion • Endoscopic US (even newer but used less) • Useful in obese patients
CT Scan of acute pancreatitis CT shows significant swelling and inflammation of the pancreas
Acute Pancreatitis • Morbidity and mortality highest if necrosis present (especially if necroctic area infected) • Dual phase CT scan useful for initial eval to look for necrosis • However, necrosis may not be present for 48-72 hours
Prognosis • Many different scoring systems • Ranson (most popular & always taught in med-school) • No association found with score, and mortality or length of hospitalization • APACHE II • CT severity Index • Recent studies show this to be most predictive of adverse outcomes • CT score > 5 associated with 15x mortality rate • Problem is 1 CT study showing this was conducted 72 hours after admission (Ranson/Apache are 24 & 48 hours) • Imrie Score • Atlanta Classification used to help compare various scores (clinical research trials)
Ranson Criteria • Admission • Age > 55 • WBC > 16,000 • Glucose > 200 • LDH > 350 • AST > 250 • During first 48 hours • Hematocrit drop > 10% • Serum calcium < 8 • Base deficit > 4.0 • Increase in BUN > 5 • Fluid sequestration > 6L • Arterial PO2 < 60 • 5% mortality risk with <2 signs • 15-20% mortality risk with 3-4 signs • 40% mortality risk with 5-6 signs • 99% mortality risk with >7 signs
CT Severity Index • CT Grade • A is normal (0 points) • B is edematous pancreas (1 point) • C is B plus extrapancreatic changes (2 points) • D is severe extrapancreatic changes plus one fluid collection (3 points) • E is multiple or extensive fluid collections (4 points) • Necrosis score • None (0 points) • < 1/3 (2 points) • > 1/3, < 1/2 (4 points) • > 1/2 (6 points) • TOTAL SCORE = CT grade + Necrosis 0-1 = 0% mortality 2-3 = 3% mortality 4-6 = 6% mortality 7-10 = 17% mortality
Therapy • Remove offending agent (if possible) • Supportive !!! #1- NPO (until pain free) • NG suction for patients with ileus or emesis • TPN may be needed #2- Aggressive volume repletion with IVF • Keep an eye on fluid balance/sequestration and electrolyte disturbances
Therapy continued # 3- Narcotic analgesics usually necessary for pain relief…textbooks say Meperidine… • NO conclusive evidence that morphine has deleterious effect on sphincter of Oddi pressure # 4- Urgent ERCP and biliary sphincterotomy within 72 hours improves outcome of severe gallstone pancreatitis • Reduced biliary sepsis, not actual improvement of pancreatic inflammation #5- Don’t forget PPI to prevent stress ulcer
Complications • Necrotizing pancreatitis • Significantly increases morbidity & mortality • Usually found on CT with IV contrast • Pseudocysts • Suggested by persistent pain or continued high amylase levels (may be present for 4-6 wks afterward) • Cyst may become infected, rupture, hemorrhage or obstruct adjacent structures • Asymptomatic, non-enlarging pseudocysts can be watched and followed with imaging • Symptomatic, rapidly enlarging or complicated pseudocysts need to be decompressed
Complications continued #2 • Infection • Many areas for concern: abscess, pancreatic necrosis, infected pseudocyst, cholangitis, and aspiration pneumonia -> SEPSIS may occur • If concerned, obtain cultures and start broad-spectrum antimicrobials (appropriate for bowel flora) • In the absence of fever or other clinical evidence for infection, prophylactic antibiotics is not indicated • Renal failure • Severe intravascular volume depletion or acute tubular necrosis may lead to ARF
Complications continued #3 • Pulmonary • Atelectasis, pleural effusion, pneumonia and ARDS can develop in severe cases • Other • Metabolic disturbances • Hypocalcemia, hypomagnesemia, hyperglycemia • GI bleeds • Stress gastritis • Fistula formation
Prognosis • 85-90% mild, self-limited • Usually resolves in 3-7 days • 10-15% severe requiring ICU admission • Mortality may approach 50% in severe cases
Chronic pancreatitis • Pathophys - irreversible parenchymal destruction leading to pancreatic dysfunction • Persistent, recurrent episodes of severe pain • Anorexia, nausea • Constipation, flatulence • Steatorrhea • Diabetes
Chronic pancreatitis • #1- etiology is chronic EtOH abuse (90%) • Gallstones • Hyperparathyroidism • Congenital malformation (pancreas divisum) • Idiopathic • MRCP of pancreas divisum
Evaluation • or normal amylase and lipase • Plain AXR / CT may show calcified pancreas • Pain management critical • EtOH cessation may improve pain • Narcotic dependency is common
Complications • Exocrine insufficiency typically manifests as weight loss and steatorrhea • If steatorrhea present, a trypsinogen level < 10 is diagnostic for chronic pancreatitis • Manage with low-fat diet and pancreatic enzyme supplements (Pancrease, Creon) • Endocrine insufficiency may result from islet cell destruction which leads to diabetes
Conclusion • Pancreatitis is common • YOU WILL SEE IT!!! • 10-15% are severe = ICU admission • Mortality may approach 50% in severe cases • These are the cases where knowing future complications would be great (ie finding a marker that correlates with severity…and that’s what the clinical researchers are attempting to do)
References • “The Washington Manual of Medical Therapeutics.” 32nd edition. 2007. Department of Medicine, Washington University School of Medicine. • Caroll JK, et al. “Acute Pancreatitis: Diagnosis, Prognosis and Treament.” American Family Physican. 2007; Vol. 75/No 10:1513-1522 • www.uptodate.com • Leung TK et al. “Balthazar CT severity index is superior to Ranson criteria and APACHE II scoring system in predicting acute pancreatitis outcome.” World J Gastroenterology. 2005; 11:6049-52. • Hatzicostas C et al. “Balthazar CT severity index is superior to Ranson criteria and APACHE II and II scoring systems.” J Clin Gastroenterology. 2003;36:253-60 • Vriens PW et al. “CT severity index is an early prognostic tool for acute pancreatitis.” J Am Coll Surgery. 2005; 201:497-502.
Malignant Exocrine Tumors Of The Pancreas Cancer pancreas & periampullary carc.
Incidence : Age :Old age : 50-70 years Sex : ♂ : ♀ = 2 :1
Aetiology : ( Risk factors) : • Cigarette smoking • DM . • Alcoholism. • Diet rich in animal fat . • Chronic pancreatitis • Benzedrine & B-naphthylamine workers
Pathology : Site : Head 70 % Head proper ( 2/3) small tumor but causes early obstruction of CBD Periampullary(1/3) ampulla of vater , distal CBD and descending duodenum . Body & Tail ( 30%) Usually The Tumor is larger and metastasizes more rapidly N.E: A poorly demarcated , greyish brown nodule
ME: Duct cell origin : 90 % Duct cell adenocacinoma , mucinous adenocarcinoma . Cystadenocarcinoma Acinar cell origin Acinar cell adenocarcinoma Cystadenocarcinoma Others: Pancreatoblastoma , CT tumors, lymphomas
Metastases Spread : Direct: Intrapancreatic,CBD , duodenum , stomach Lymphatic : • LN along the hepatic artery ( ca. head ) • Gastric ,celiac, mesenteric and Para aortic LN ( ca. body & tail ) • Finally → portahepatis LN, supra clavicular LN • Blood spread :to liver , lungs , adrenal gl. Bone, brain, skin • Peritoneal seeding :common with ca body & tail .
Complications : Obstruction: • Portal vein or splenic vein → splenomegaly & varices • Hepatic veins → Budd Chiari Syndrome . • I.V.C → cyanosis & leg oedema • CBD→ obst. jaundice
Duodenum or stomach → Gastric outlet obstruction • Ulcerationinto stomach or duodenum →heamatemesis or melena • Infiltrationof peripancreatic nerves → pain
C.P. : *Symptoms: Jaundice: • It is a manifestation of cancer head. Causes: • Obstruction of CBD by the tumor or portahepatis LN. • Liver secondaries. • It is progressive but may be intermittent in ampullary carcinoma due to sloughing of a part of the tumor . • The old belief that jaundice in cancer head is painless is no more valid.
Pain: • It is the most common initial symptom. • Causes: • Retroperitoneal extension. • Distension of an obstructed pancreatic or CBD. • It may be felt in the epigastrium, right or left hypochandria, or in the back. • It is first dull aching in nature, it may be episodic and related to meals. Later on, it may become severe and boring (constant) • It is exaggerated by lying supine and relived by leaning forwards.
Pancreatic asthenia (wt loss+ lassitude+ cachexia) • Causes: • Anorexia • Anxiety associated with undiagnosed illness. • D.M • Biliary obstruction with malabsorption. • Hepatocellular dysfunction.
Non specific symptoms : The earliest symptoms of ca pancreas are nausea, epigastric bloating, change in bowel habits and vomiting.
Picture of complications * Examination : A - General examination: • General condition: bad in most cases. • Jaundice • Fever and tachycardia: =cholangitis. • Anaemia. • Migratory thrombophlebitis ( Trausseau sign ): in 10% of cases .It is not pathognomonic & could occur with any advanced cancer. • Leg oedema: IVC obstruction
B- Abdominal examination: • Hepatomegaly: Hydrohepatosis- secondaries. • Enlarged GB: (65%) according to Courvoisier's law. • Abdominal tenderness. • Palpable epigastric mass: hard and fixed ( rare finding) • Ascites : malignant ascites or portal vein compression • Sister – Joseph's nodule.
Investigations: Laboratory investigations • Urine analysis • Stool analysis • Occult Blood In Stool • Silver stools ( acholic stool mixed with blood ) • ↓Stercobilinogen
L.F.T. • Glucose tolerance test • CBC: Anaemia ,Leucocytosis 1-Radiological • Barium meal • Widening of the duodenal loop < C- shaped > The reversed – 3 sign
2-U.S : Dilated CBD, Liver secondaries ,The tumor 3-EUS (Endoscopic U.S) : Good visualization of the tumor ,vascular invasion 4-CT scan: * Local extent of the tumor *Local vascular invasion * Metastases *Allows CT-guided biopsy 5- MRI It can differentiate malignant from inflammatory masses 6-MRCP
7. Angiography: (its use is replaced by CT scan) C- Endoscopy (ERCP) • Visualization of the lesion (periampullary- duodenal invasion) • Cholangiogram & pancreaticogram→ • The lesion • The pancreatic duct • CBD