Pancreas CANCER
730 likes | 1.22k Vues
Pancreas CANCER. Clinical manifestations, diagnosis, and staging of exocrine pancreatic cancer Pathology of exocrine pancreatic neoplasms Epidemiology and risk factors for exocrine pancreatic cancer Molecular pathogenesis of exocrine pancreatic cancer

Pancreas CANCER
E N D
Presentation Transcript
Clinical manifestations, diagnosis, and staging of exocrine pancreatic cancer • Pathology of exocrine pancreatic neoplasms • Epidemiology and risk factors for exocrine pancreatic cancer • Molecular pathogenesis of exocrine pancreatic cancer • Endoscopic ultrasound in the staging of exocrine pancreatic cancer • Surgery in the treatment of exocrine pancreatic cancer and prognosis • Adjuvant and neoadjuvant therapy for exocrine pancreatic cancer • Chemotherapy for advanced exocrine pancreatic cancer • Management of locally advanced and borderline resectable exocrine pancreatic cancer • Exocrine pancreatic cancer: Palliation of symptoms Pancreas Exocrin Cancer
Epidemiology and risk factors for exocrine pancreatic cancer • Molecular pathogenesis of exocrine pancreatic cancer • Endoscopic ultrasound in the staging of exocrine pancreatic cancer • Surgery in the treatment of exocrine pancreatic cancer and prognosis • Adjuvant and neoadjuvant therapy for exocrine pancreatic cancer • Chemotherapy for advanced exocrine pancreatic cancer • Management of locally advanced and borderline resectable exocrine pancreatic cancer • Exocrine pancreatic cancer: Palliation of symptoms Pancreas Exocrin Cancer
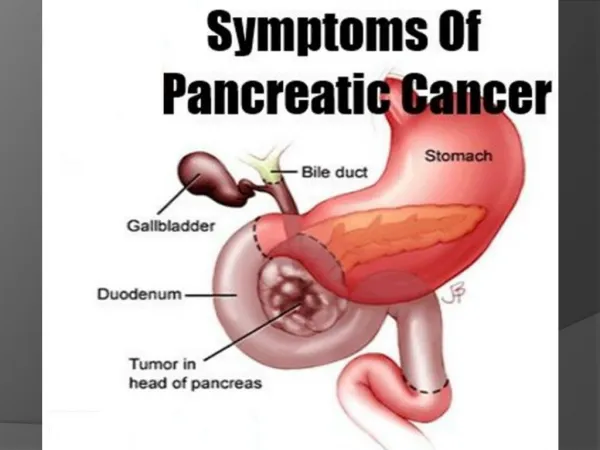
The commonly used term "pancreatic cancer" usually refers to a ductal adenocarcinoma of the pancreas (including its subtypes). • More than 95 percent of malignant neoplasms of the pancreas arise from the exocrine elements and are referred to as exocrine pancreatic cancers. (See 'Pathology' above.) Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
cancer of the exocrine pancreas • almost all are expected to die from the disease • Surgical resection offers the only chance of cure • Only 15 to 20 percent of patients have resectable disease at diagnosis; • approximately 40 percent have metastatic disease, • and another 30 to 40 percent have locally advanced unresectable tumors. • Median survival is 8 to 12 months for patients with locally advanced disease and less for those with metastatic disease at presentation. Management of locally advanced and borderline resectable exocrine pancreatic cancer
The most common presenting symptoms in patients with exocrine pancreatic cancer are • pain, • jaundice, and • weight loss. • Compared to tumors in the body and tail of the gland, pancreatic head tumors more often present with jaundice, steatorrhea, and weight loss. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
Patients who present with jaundice or epigastric pain and weight loss often undergo right upper quadrant transabdominal ultrasound initially to evaluate for dilated bile ducts or a pancreatic mass. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
In the jaundiced patient, • ultrasoundis highly sensitive for • detecting biliary tract dilation and • establishing the level of obstruction; • it is highly sensitive for pancreatic masses >3 cm. • Endoscopic retrograde cholangiopancreatography (ERCP) • is a highly sensitive tool for visualization of the biliary tree and pancreatic ducts in patients with jaundice. • However, the role of ERCP in patients with suspected pancreatic cancer is evolving into a mainly therapeutic rather than diagnostic modality in patients who present with cholestasis due to tumor obstruction of the biliary system. • An alternative approach is magnetic resonance cholangiopancreatography (MRCP). • is generally reserved for patients with gastric outlet or duodenal stenosis, • or who have had surgical rearrangement (eg, Billroth II) • or ductal disruption, resulting in ducts that are difficult to assess successfully by ERCP, in the setting of chronic pancreatitis, • or for patients in whom attempted ERCP is either totally unsuccessful or provides incomplete information because of pancreatic duct obstruction. . Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
For patients with epigastric pain and weight loss without jaundice, • in whom the differential diagnosis includes pancreatitis, transabdominal ultrasound is not the preferred initial test because it is associated with a high frequency of incomplete examinations owing to overlying bowel gas due to ileus, and it cannot clearly identify necrosis within the pancreas; these important findings are best seen by contrast enhanced CT scan. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
Endoscopic ultrasound (EUS) may be of use in a patient who is suspected of having pancreatic cancer based upon the clinical presentation of jaundice, unexplained upper abdominal pain/weight loss, or an unexplained episode of pancreatitis, but who has no evidence of a mass lesion on initial transabdominal ultrasound or CT. • Given the limited sensitivity and specificity, the serum tumor marker CA 19-9 should not be used as a diagnostic test for pancreatic cancer. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
Histologic confirmation is required to establish a diagnosis of pancreatic cancer. • Biopsy of a pancreatic mass can be accomplished through percutaneous or endoscopic approaches. • However, not all patients require a preoperative biopsy, • and the next step in the workup of a patient with suspected pancreatic cancer is often a staging evaluation to establish disease extent and resectabilityrather than biopsy. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
When a mass lesion of the pancreas is detected on CT or ultrasound, • it is reasonable to conclude that a neoplasm (most likely malignant) is present, and triple-phase, contrast enhanced helical (preferably multidetector row) CT is an appropriate next step to assess disease extent and resectability. • Local unresectabilityis usually (but not always) due to • vascular invasion, particularly of the superior mesenteric artery (SMA). • Endoscopic ultrasound (EUS) is another effective method to assess tumor extent and vascular invasion, • but we generally prefer CT given its greater utility in assessing for distant metastases. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
Although practice is variable, most surgeons would consider a pancreatic cancer to be categorically unresectable if any of the following are present: • Extensive peripancreaticlymphatic involvement, nodal involvement beyond the peripancreatic tissues, and/or distant metastases. • Direct involvement of the superior mesenteric artery (SMA), inferior vena cava, aorta, celiac axis, or hepatic artery, • as defined by the absence of a fat plane between the low density tumor and these structures on CT scan. • Encasement (more than one-half of the vessel circumference) • or occlusion/thrombus of the superior mesenteric vein (SMV) or the SMV-portal vein confluence used to be universally considered an indicator of unresectability. • However, many centers have demonstrated the feasibility of SMV reconstruction, and this is now considered by many to represent borderline resectable disease; in practice, most of these patients are referred for neoadjuvanttherapy prior to surgery. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
The utility of PET scans, chest CT, and MRI in the staging workup of suspected pancreatic cancer, particularly whether any of these imaging studies provides information beyond that obtained by triple-phase, contrast enhanced helical multidetector row CT remains uncertain, and we do not routinely order these tests Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
Assessment of serum levels of the tumor marker CA 19-9 prior to surgery and following resection, if elevated, is valuable to assist in prognostication. • In addition, serial monitoring of CA 19-9 levels, if initially elevated, is useful to follow patients after potentially curative surgery and for those who are receiving chemotherapy for advanced disease. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
Our general diagnostic approach, as detailed in the following sections, is summarized in the algorithm ( algorithm 2 ). In general: • Tissue diagnosis is mandatory for patients who are • unfit to undergo a major resection, • for those with a high suspicion of metastatic disease, • and for any patient being considered for neoadjuvant therapy because of locally advanced nonmetastatic disease. • EUS-guided FNA is the best modality for obtaining a tissue diagnosis, even if the tumor is poorly visualized by other imaging modalities. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
If a patient is a reasonable surgical candidate, and if the clinical presentation and imaging are typical for a resectableadenocarcinoma, it is reasonable to proceed to surgery without a tissue diagnosis. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
For jaundiced patients with no involvement or minimal involvement of the major vessels and no evidence of distant metastases on radiographic imaging, • we proceed directly to open laparotomy. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
For non-jaundiced patients (including all those with body or tail tumors), as well as those with major but incomplete involvement of the vascular structures (eg, tumor contiguous to less than one-half of the vessel circumference), • we perform preoperative laparoscopy to exclude tiny metastases that might have been overlooked by CT. • If the laparoscopy is negative, we then proceed to open laparotomy to assess resectability. • Other indications for a staging laparoscopy prior to open laparotomy include • a high preoperative CA 19-9 level (>1000 units/mL) • and any patient for whom high-quality imaging is in any way suggestive of occult metastatic disease. Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
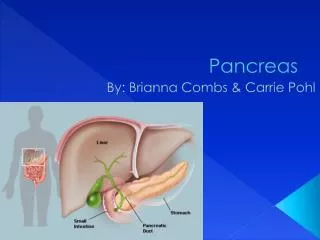
Pathology of exocrine pancreatic neoplasms Pancreas Exocrin CancerClinical manifestations, diagnosis, and staging of exocrine pancreatic cancer
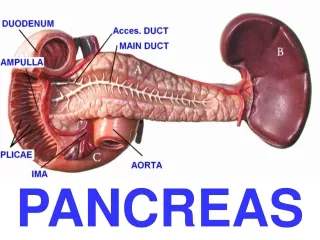
The pancreas gives rise to several malignant and benign neoplasms. • The most common benign pancreatic neoplasm is serous cystadenoma. • Several neoplasms formerly classified as benign are now accorded “premalignant” status because it is considered that some will progress to malignancy. • These include • low-grade intraductal mucinous papillary neoplasm (IPMN) • mucinous cystic neoplasm (MCN). Pancreas Exocrin CancerPathology of exocrine pancreatic neoplasms
A number of types of malignant tumors arise in the exocrine pancreas. • The commonly used term "carcinoma of the pancreas" or "pancreatic cancer" usually refers to ductal adenocarcinoma, which represents about 85 percent of all pancreatic neoplasms. • The more inclusive term "exocrine pancreatic neoplasms" includes all tumors that are related to the pancreatic ductal and acinar cells and their stem cells. • More than 95 percent of malignant neoplasms of the pancreas arise from the exocrine elements. • The remainder arise from the endocrine elements within the pancreas (the islet cells). Pancreas Exocrin CancerPathology of exocrine pancreatic neoplasms
The major risk factors for pancreatic cancer are: • Cigarette smoking . • High body mass and lack of physical activity • Nonhereditary chronic pancreatitis • A role for familial aggregation and/or genetic factors is suggested by the fact that 5 to 10 percent of patients with pancreatic cancer have a first degree relative with the disease . • Hereditary pancreatitis is an autosomal dominant disorder that accounts for a small fraction of cases of chronic pancreatitis. • The majority of affected individuals develop symptoms before the age of 20 and often before the age of five . • Germline mutations in known cancer-causing genes, such as BRCA1, BRCA2, and STK11 (the gene mutated in Peutz-Jeghers syndrome) are associated with an increased risk of pancreatic cancer • Ataxia-telangiectasia is associated with an increased risk of pancreatic cancer . Pancreas Exocrin CancerEpidemiology and risk factors for exocrine pancreatic cancer
The optimal timing and frequency of screening for pancreatic cancer in individuals at elevated risk is uncertain. • Some expert groups recommend screening for high-risk individuals who have a 5 or 10-fold or higher risk of pancreatic cancer ( table 2 ) . • The optimal time to begin screening is unclear, but some groups recommend beginning at age 40 for those with hereditary pancreatitis and 10 years before the age at which pancreatic cancer was first diagnosed in individuals with an inherited predisposition. • In patients with PJS, screening for pancreatic cancer is recommended at age 30 years. • There is no consensus on the appropriate interval for screening and also no consensus as to the optimal screening strategy. Pancreas Exocrin CancerEpidemiology and risk factors for exocrine pancreatic cancer
Potential candidates for screening for pancreatic cancer Pancreas Exocrin CancerEpidemiology and risk factors for exocrine pancreatic cancer
Cancer of the exocrine pancreas is associated with a poor prognosis, even if a complete (R0) resection can be accomplished. • Systemic chemotherapy, radiation therapy (RT), and a combination of chemotherapy and RT have all been applied following surgery in an effort to improve cure rates. • Although the benefit of adjuvant therapy has become clearer in recent years, the optimal choice of treatment modality (chemotherapy with or without RT) remains intensely controversial. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
There is no consensus regarding the optimal management of patients after resection of an exocrine pancreatic cancer, and the approach is different in Europe and in the United States: • Largely based upon • the ESPAC-1 trial, which showed that 5-FU-containing chemotherapy prolongs survival, • and results of the German CONKO trial showing a survival benefit from adjuvant gemcitabine • most European clinicians use chemotherapy alone after resection of a pancreatic neoplasm. • Where available, oral therapy with S-1 represents an appropriate alternative to gemcitabine monotherapy. • The American approach more often includes • chemoradiotherapyas well as adjuvant chemotherapy. • Guidelines from the NCCN support either approach. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
The following represents approach to patients with resected pancreatic tumors. • Eligible patients should be encouraged to enroll in clinical trials evaluating the potential benefits of chemotherapy and/or chemoradiotherapy as well as new therapies. Continue Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
The following represents approach to patients with resected pancreatic tumors. • Off-protocol, we suggest a combination of concurrent chemoradiotherapy and chemotherapy for all patients with resected pancreatic cancer ( Grade 2B ). • During the concurrent chemoradiotherapyportion, we prefer infusional5-FU, and we use gemcitabine alone for the chemotherapy portion. Continue Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
The following represents approach to patients with resected pancreatic tumors. • The optimal way to sequence 5-FU-based chemoradiotherapy and gemcitabine chemotherapy is unclear. An acceptable regimen is that used in RTOG 9704 [ 38 ], which consists of • three weekly doses of gemcitabine alone (1000 mg/m 2 per week), • followed by chemoradiotherapy using concurrent infusional 5-FU. • Although the RTOG trial used 250 mg/m 2 daily continuously, many clinicians, including our group, consider this too toxic and use 225 mg/m 2 daily, five days per week. • Following chemoradiotherapy and starting three to five weeks later, three months of single agent gemcitabine ( table 2 ) are given. (See 'Gemcitabine-based approaches' above and "Treatment protocols for pancreatic cancer" .) Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
Although neoadjuvantchemoradiotherapy can be safely delivered to patients with localized pancreatic cancer, no study has clearly demonstrated improved resectability or survival, and it remains unclear whether this approach provides comparable benefit to adjuvant (postoperative) therapy. • We suggest not administering neoadjuvantchemoradiotherapy outside of clinical trials at present (Grade2C ). • Eligible patients should be encouraged to enroll on clinical trials testing this strategy. (See'Neoadjuvanttherapy for potentially resectable tumors' above.) Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
GITSG study • observation or • external beam RT (EBRT, 40 Gy) plus concurrent bolus 5-FU (500 mg/m 2 per day on the first three and last three days of RT), • followed by maintenance chemotherapy (5-FU 500 mg/m 2 per day for three days monthly) for two years or until disease progression • patients receiving postoperative chemoradiotherapy had significantly longer median overall survival (20 versus 11 months) and a doubling of the two-year survival rate (20 versus 10 percent) Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
EORTC study • postoperative concurrent 5-FU (25 mg/kg per day by continuous infusion) plus EBRT (40 Gy in split courses) • or observation • In contrast to the GITSG findings, postoperative chemoradiotherapy did not significantly improve median overall survival or two-year survival (26 versus 34 percent for control and treated patients, respectively, p = 0.099 Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
ESPAC-1 trial • 2x2 factorial design in which the relative benefits of • adjuvant chemotherapy, • chemoradiotherapy, or • chemoradiotherapyfollowed by chemotherapy • observation alone chemoradiotherapy consisted of 20 Gy EBRT plus three days of concomitant 5-FU, repeated after a planned break of two weeks. adjuvant chemotherapy consisted of bolus leucovorin-modulated 5-FU (leucovorin 20 mg/m 2 , 5-FU 425 mg/m 2 ), administered daily for five days, every 28 days, for six months. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
ESPAC-1 trial Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
ESPAC-1 trial Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
ESPAC-1 trial • This analysis was criticized for the following reasons: • Patients and clinicians were allowed to select which trial to enter, raising concerns as to generalizability and the appropriateness of combining results. • Clinicians were allowed, according to their own preferences, to deliver "background" chemoradiation or chemotherapy. • Comparisons of treatment groups that were pooled together by treatment actually received, rather than "intent-to-treat" analysis, resulted in nearly one-third of the "no chemotherapy" and "chemotherapy alone" patients receiving chemoradiotherapy. • Similar to the EORTC trial discussed above, the chemoradiotherapy group received RT in a split course fashion, and the final dose (ranging from 40 to 60 Gy) was left to the judgment of the treating physician. • The chemoradiotherapy group did not include postradiotherapy adjuvant chemotherapy; thus, the results cannot be directly compared to the results of the GITSG trial. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
Chemotherapy only • Gemcitabine • CONKO trial • 368 patients with grossly complete (R0 or R1) surgical resection and a preoperative CA 19-9 level <2.5 times the upper limit of normal • gemcitabine (1000 mg/m 2 days 1, 8, and 15 every four weeks for six months) or no treatment after surgery • significantly longer median DFS (13.4 versus 6.9 months), • which was evident in those with • negative nodes (24.8 versus 10.4 months) and • positive (12.1 versus 6.4 months), • as well as those with negative margins (13.1 versus 7.3 months) or • positive (15.8 versus 5.5 months). • ASCO meeting, there was also a modest but significant improvement overall survival that favored gemcitabine (median 22.8 versus 20.2 months, p = 0.005, five-year survival 21 versus 9 percent) Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
Chemotherapy only • Gemcitabine versus a fluoropyrimidine • ESPAC-3trial • 1088 patients with resected exocrine pancreatic cancer to • six months of postoperative adjuvant treatment with either gemcitabine (1000 mg/m 2 weekly for three of every four weeks) or • leucovorinmodulated 5-FU (leucovorin 20 mg/m 2 followed by 5-FU 425 mg/m 2 IV bolus days 1 through 5, every 28 days) [ 46 ] • At a median follow-up of 34 months, median survival was similar (23.6 versus 23 months with gemcitabine and fluoropyrimidine therapy, respectively). • the patients assigned to 5-FU/leucovorin had more grade 3 to 4 treatment-related toxicity • Given this safety profile, gemcitabine is the preferred agent when compared with monthly bolus (Mayo Clinic) 5-FU/LV. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
Chemotherapy only • Gemcitabine versus a fluoropyrimidine • ESPAC-3trial • 1088 patients with resected exocrine pancreatic cancer to • six months of postoperative adjuvant treatment with either gemcitabine (1000 mg/m 2 weekly for three of every four weeks) or • leucovorinmodulated 5-FU (leucovorin 20 mg/m 2 followed by 5-FU 425 mg/m 2 IV bolus days 1 through 5, every 28 days) [ 46 ] • At a median follow-up of 34 months, median survival was similar (23.6 versus 23 months with gemcitabine and fluoropyrimidine therapy, respectively). • the patients assigned to 5-FU/leucovorin had more grade 3 to 4 treatment-related toxicity • Given this safety profile, gemcitabine is the preferred agent when compared with monthly bolus (Mayo Clinic) 5-FU/LV. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
Chemotherapy only • Gemcitabine versus a fluoropyrimidine • Gemcitabine versus S-1 • three different agents: ftorafur, chlorohydroxydihydropyridine (a potent inhibitor of DPD [dihydropyrimidine dehydrogenase]) • S-1 (40 to 60 mg twice daily for four weeks and repeated every six weeks for four courses) • In a preliminary report presented at the 2013 ASCO Gastrointestinal Cancers Symposium, S-1 was not inferior to gemcitabine • S-1 represents a reasonable and more convenient alternative to gemcitabine when adjuvant chemotherapy alone is recommended following resection of a pancreatic cancer. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
Chemotherapy versus chemoradiotherapy Two good design Trail • ESPAC-1 trial, • EORTC 40013/FFCD-9203/GERCOR phase II study • Ninety patients with resected pancreatic cancer (70 percent node-positive, 97 percent completely resected [R0]) were randomly assigned to gemcitabine -based chemoradiotherapy (two cycles of weekly gemcitabine alone [1000 mg/m 2 weekly, three weeks on, one week off]) followed by RT (50.4 Gy in 28 daily 1.8 Gy fractions) with concurrent gemcitabine (300 mg/m 2 once weekly four hours before RT for five to six weeks), or a control group. • Initially the control group was observation alone (n = 4), but the protocol was amended, and the remainder of the control group (n = 41) received four cycles of gemcitabine alone (1000 mg/m 2 for three consecutive weeks followed by a one week rest). Treatment started within eight weeks of surgery. • chemoradiotherapy was not deleterious; median DFS was 12 versus 11 months in the control group, and median overall survival was 24 months in both arms. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
Chemotherapy versus chemoradiotherapy Two good design Trail • ESPAC-1 trial, • EORTC 40013/FFCD-9203/GERCOR phase II study • Ninety patients with resected pancreatic cancer (70 percent node-positive, 97 percent completely resected [R0]) were randomly assigned to gemcitabine -based chemoradiotherapy (two cycles of weekly gemcitabine alone [1000 mg/m 2 weekly, three weeks on, one week off]) followed by RT (50.4 Gy in 28 daily 1.8 Gy fractions) with concurrent gemcitabine (300 mg/m 2 once weekly four hours before RT for five to six weeks), or a control group. • Initially the control group was observation alone (n = 4), but the protocol was amended, and the remainder of the control group (n = 41) received four cycles of gemcitabine alone (1000 mg/m 2 for three consecutive weeks followed by a one week rest). Treatment started within eight weeks of surgery. • chemoradiotherapy was not deleterious; median DFS was 12 versus 11 months in the control group, and median overall survival was 24 months in both arms. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
Radiation therapy alone • Few data address the benefit of adjuvant EBRT alone after potentially curative surgery • intraoperative RT (IORT) in conjunction with surgical resection??? • Most trials have combined IORT with preoperative EBRT and chemotherapy (see below); none are randomized with a control group of resection without IORT. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
Summery for adj CCR Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
There is no consensus regarding the optimal management of patients following resection of pancreatic cancer, and the approach is different in Europe and in the United States. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
The European approach • emphasizes the weaknesses of the early GITSG study and the lack of data demonstrating a significant survival benefit with chemoradiotherapy in the EORTC and ESPAC-1 trials. • Most European clinicians support the conclusions of the ESPAC-1 trial (ie, that chemotherapy prolongs survival and chemoradiotherapy may actually worsen survival). • The benefit of adjuvant chemotherapy alone is further supported by the German CONKO trial [ 40 ]. • Guidelines for treatment of pancreatic adenocarcinoma from the European Society of Medical Oncology suggest that chemoradiotherapy in the adjuvant setting should only be performed within the context of a randomized controlled trial [ 56 ] Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
The American approach to adjuvant therapy differs with regard to the benefit of chemoradiotherapy and emphasizes the following points: • The high risk of local failure and potential for benefit from chemoradiotherapy • The high rate of positive retroperitoneal margins and the impact of this finding on survival • The survival benefit from chemoradiotherapy in the GITSG study • The trend toward improved survival seen with chemoradiotherapy in the underpowered EORTC study • The serious design flaws of the ESPAC-1 trial and the inherent difficulty in drawing definitive conclusions from this study Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer
In the opinion of the uptodateand NCCN , • patients who have undergone resection of an exocrine pancreatic cancer should be encouraged to enroll in clinical trials evaluating the potential benefits of chemotherapy and/or chemoradiotherapy as well as new therapies. • As an example, RTOG trial 0848 is a phase III trial examining the benefit of adding erlotinibto adjuvant gemcitabine with or without subsequent fluoropyrimidine-based chemoradiotherapy in patients with resected tumors of the head of the pancreas [ 57 ]. Pancreas ExocrinCancerAdjuvant and neoadjuvant therapy for exocrine pancreatic cancer