Download
1 / 4

E N D
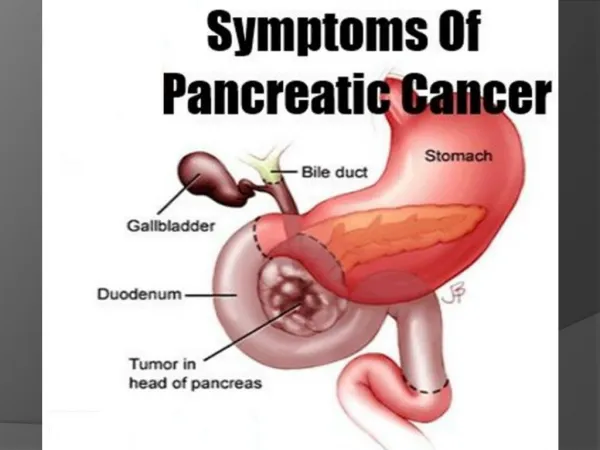
Pancreas Cancer (Body & Tail) gicancerindia.com/pancreas-cancer-body-tail/ The pancreatic cancer is one of the most aggressive cancers of the digestive tract. Cancer arising in the body & tail of pancreas are larger, more frequently metastasized and less often resectable in comparison to the cancer arising in head of pancreas. However with recent developments the surgery for pancreatic cancer is safer than ever before. Moreover newer chemotherapy agents and improvement in radiation therapy has led to less toxicity and improved survival. Our team is in forefront of pancreatic cancer surgery and research with presentations and publications in top international journals. What are the symptoms? pancreas cancer (body & tail ) The tumors of the pancreatic body & tail often do not cause any specific symptoms in the early stage. Pain in abdomen or back, unexplained weight loss, recent onset diabetes and palpable abdominal mass are the characteristic symptoms but are often vague. In most instances by the time patient develops these symptoms often they have already reached an advanced stage and cancer has spread beyond the pancreas. 1/4
However having these symptoms does not mean that you have cancer pancreas but you should see your doctor so that the cause for these symptoms can be diagnosed. What is the preoperative work up? Details of your symptoms, other relevant medical history and information regarding probable risk factors including smoking and family history is an important part of the work up. Subsequently based on these information and physical examination your doctor may recommend investigations to reach a diagnosis. The objectives of investigations for a patient with suspected cancer involving this region are: 1. Establish the diagnosis 2. Assess fitness for major surgery 3. Meticulous preoperative staging to select patients who are more likely to benefit from surgery A triple phase contrast enhanced CT scan of the whole abdomen (pancreas protocol) is the preferred imaging investigation. Contrast enhanced MRI may also be used for staging purposes. CT or MRI scan provide details of the tumor such as size, location of tumor & its relationship with major blood vessels. Also the spread of tumor beyond pancreas to liver, lymph nodes or peritoneum can be assessed. In patients with resectable tumors high resolution CT scan of chest with or without contrast is done to exclude spread of cancer deposits in lungs. Positron emission tomography (PET) scan also is indicated in selected patients. However it is important to note that PET scan is not a substitute for triple phase pancreas protocol CT scan. Is there a role for preoperative tissue diagnosis / FNAC? Preoperative tissue diagnosis is not needed in all patients prior to surgery. Based on imaging results if your doctor believes that the tumor is very likely to be pancreatic cancer and complete removal of the cancer is feasible with surgery then tissue diagnosis is not mandatory. However endoscopic ultrasound may be performed for fine needle aspiration cytology (FNAC), when the tumor has doubtful resectability, plan for neoadjuvant therapy or for characterization of rare tumors. Also for patients with spread of cancer beyond pancreas FNAC or biopsy is required prior to starting the chemotherapy. What is the role of tumor markers for the diagnosis of these cancers? The tumor markers for these cancers include CA 19-9 & CEA. These have no role for confirmation of diagnosis. However baseline values have a role in subsequent follow up. What is meant by stages of the cancer pancreas? 2/4
The most widely used staging system for cancer pancreas is American Joint Committee on cancer (AJCC) staging system which includes TNM classification of the cancer. The TNM system indicates size of the tumor (T), lymph node involvement (N) and distant metastases to lymph nodes outside specified regional nodes or other organs (M). The stage of the cancer indicates the advancement of the cancer in terms of resectability of the cancer and likely survival. Stage I & II cancers: resectable Stage III (borderline resectable): resectable Stage III cancers (locally advanced): unresectable Stage IV cancers: cancer has spread beyond regional tissues: unresectable What are the treatment options? a. Curative surgery Distal pancreatectomy with splenectomy and regional lymphadenectomy remains the only available curative treatment for cancer of pancreas of body and tail that is consistent with long term survival. The surgery can be performed by traditional open surgery or by minimally invasive techniques (laparoscopic or robot assisted). At specialized centers, the procedure can now be accomplished with a mortality rate ranging between 1 to 4% however postoperative morbidity continues to be substantial (up 20 to 40%). b. Palliative management In patients where curative surgery is not feasible because of the spread of cancer to other organs or peritoneal metastases surgical gastro-jejunostomy is an acceptable palliative procedures for tumors infiltrating the small intestine at duodeno-jejunal flexure. What is meant by pancreatic fistula after surgery? Pancreatic fistula means leak of pancreatic juice from the stump of remaining pancreas following surgery. It is the commonest complication following surgery and is significant because it may lead to abscess, sepsis or major bleeding. What are the recent advancements for surgery of cancer pancreas? Radical antegrade modular pancreatosplenectomy (RAMPS) – high level evidence supporting prolonged overall survival is still lacking, however it has been shown to be oncologically superior in terms of increased number of lymph node harvest and greater R0 resection rates. Is surgery feasible for locally advanced cancer of pancreas involving celiac axis? 3/4
Celiac axis is the main vessel supplying blood to stomach, liver, pancreas & spleen. Pancreatic cancer involving celiac axis are considered unresectable by most guidelines. However selected patients can undergo distal pancreatectomy with celiac axis resection (modified Appleby procedure) with acceptable morbidity and mortality (5-18%). With modified Appleby procedure median overall survival is 15-25 months in this subset of patients with advanced cancer. What are the outcomes following curative surgery? The patients who do undergo curative surgery with surgical margins free of tumor have 5- year overall survival up to 20%. Margin positive resection confers no survival advantage and has an outcome similar to that of local unresectable disease. Which patients need chemotherapy following curative surgery? Patients in whom the disease has spread to lymph nodes on final histopathological examination of surgical specimen are likely to benefit from chemotherapy. TAGS: Pancreas Cancer treatment in Delhi, Best Pancreas Cancer treatment in Delhi, Best treatment of Pancreas Cancer in Delhi, Treatment of Pancreas Cancer in Delhi 4/4