Acute Mesenteric Ischemia
Acute Mesenteric Ischemia. Isaac George, MD Resident in Surgery Department of Surgery Columbia University College of Physicians and Surgeons. Acute Mesenteric Ischemia. Incidence Pathophysiology Diagnosis Therapy Treatment Algorithm Objectives. Objectives. Understand pathophysiology


Acute Mesenteric Ischemia
E N D
Presentation Transcript
Acute Mesenteric Ischemia Isaac George, MD Resident in Surgery Department of Surgery Columbia University College of Physicians and Surgeons
Acute Mesenteric Ischemia • Incidence • Pathophysiology • Diagnosis • Therapy • Treatment Algorithm • Objectives
Objectives • Understand pathophysiology • Identify patients at high-risk for mesenteric ischemia • Develop treatment plan for each patient/apply treatment algorithm
Introduction • Cokkinis (1921): “occlusion of the mesenteric vessels is regarded as one of those conditions of which the diagnosis is impossible, the prognosis hopeless, and the treatment almost useless.” • Occlusive or non-occlusive mechanism leading to hypoperfusion of one or more mesenteric vessels
Rationale • Incidence • 1-2/1000 hospital admissions • 1% of GI admissions1 • Mortality • 1960’s - 70-100%2 • 1970’s - 60-70%3 • Morbidity • Cardiopulmonary, MOSF • Extended LOS, TPN dependence4 • Recurrence • Up to 60%4 1 Ann Surg 2001;233(6):801-808 2 Ann Surg 1982;195:554-565 3 Ann Surg 1978;188;721-731 4 Ann Vasc Surg 2003;17:72-9
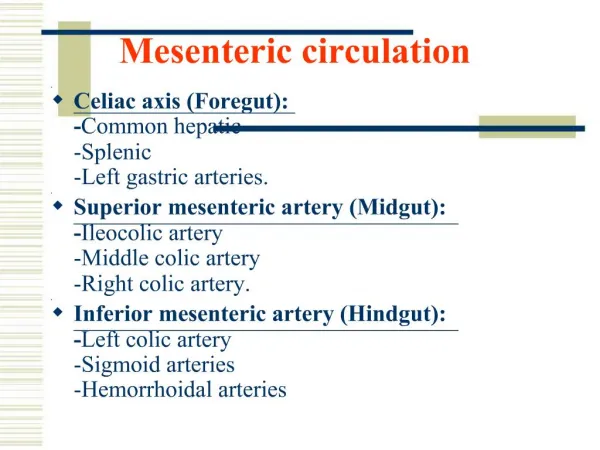
Pathophysiology: Etiology • Arterial Embolic Disease • Arterial Thrombotic Disease • Venous Thrombotic Disease • Non-occlusive Mesenteric Ischemia
Pathophysiology Arterial Embolism • Majority of cases (>50%): SMA occlusion • Location: origin of middle colic artery (ischemia from proximal jejunem to splenic flexure) • Embolic sources: cardiac (80%)1, aortic plaques • Celiac and IMA occlusion usually tolerated • SMA occlusion → death • Most have underlying stenoses as well 1 Ann Vasc Surg 1990;4:112-116
Pathophysiology Arterial Thrombotic Disease • 15% of acute intestinal ischemia1 • Pre-existing atherosclerotic disease • Worsening chronic mesenteric ischemia • Found at ostium of SMA • More delayed onset of symptoms 1 Vasc Surg 1996; 4th ed.
Pathophysiology Venous Thrombotic disease • 5-10% of intestinal ischemia • Younger patient population • 80% have hypercoaguable state • Risk factors: oral contraceptives, previous DVT/PE, malignancy, portal HTN, nephrotic syndrome • May limit arterial flow→edema, segmental infarction
Pathophysiology Non-Occlusive disease • 20-30% of acute intestinal ischemia • Response to systemic hypoperfusion • Sympathetic adrenergic system mediated • Visceral vasoconstriction/shunting for cerebral protection • Causes: any severe systemic illness, CHF, dehydration, drugs (cocaine, ergot alkaloids, digitalis, β-blockers,α-agonist, epo), hemodialysis
Arterial Thromboembolic, Non-Occlusive Severe abdominal pain Sudden onset Venous Thrombotic Less severe pain Subacute Clinical Presentation:Physical Examination • Symptoms variable • Abdominal pain-non-specific, crampy vs. steady, anterior • Gastric emptying/vomiting • Peritonitis late • Hypotension, tachycardia
Clinical Presentation: Laboratory Limited clinical utility • arterial lactate1 • amylase2 • CK, CK-BB3 • Serum phosphate4 • Other useless markers: LDH, PAF, TNF-α, AP, AST/ALT, α-glutathione 1 Eur J Surg 1994;160:381-4 2 Br J Surg 1986;73:219-21 3 Dig Dis Sci 1991;36:1589-93 4 Br J Surg 1982;69:S52-3
Clinical Presentation: Risk Factors J Vasc Surg 2002;35:445-52
Clinical Presentation: Risk factors Ann Surg 2001;233(6):801-808
Clinical Presentation: Risk factors Ann Surg 2001;233(6):801-808
Clinical Presentation Ann Vasc Surg 2003;17:72-79
Clinical Presentation Ann Surg 2001;233(6):801-808
Diagnosis: Non-Invasive Imaging X-ray Computed Tomography (helical/angiography) Ultrasound MRI/MRA
Diagnosis: X-Ray Plain Films • pneumatosis • portal venous gas • thumbprinting → • Findings late, associated with high mortality
Diagnosis: Computed Tomography Criteria • pneumatosis • venous gas • SMA/celiac/IMA occlusion w/distal disease • arterial embolism OR • bowel wall thickening + one of following: • lack of bowel wall enhancement • solid organ infarction • venous thrombosis Sensitivity: 96% Specificity: 94% 1 Radiol 2003;229:91-98
Computed Tomography Radiol 2003;229:91-98
Computed Tomography Radiol 2003;229:91-98
Computed Tomography Radiol 2003;229:91-98
Volume Rendering:Normal RG 2002;22:161-172
Volume Rendering:Ischemia RG 2002;22:161-172
Diagnosis: Ultrasound High-grade stenosis or occlusion of SMA • Sensitivity for SMA stenosis: 96% (1993) 1 • Prospective, n=100 • Surgically confirmed embolism/thrombus • Sensitivity for SMA stenosis/occlusion: 100% (1999)2 • Specificity: 98% • PPV: 93%, NPV: 100% • N=82, prospective • Confirmed with angiography 1 J Vasc Surg 1993;17:780-788 2 Radiol 1999;211:405-410
Diagnosis: MRI • Poor delineation of smaller vessels • Limited clinical application • Perfusion flow contrast studies show promise1 1 Radiol 2004;234:569-575
Diagnosis: Angiography • Gold Standard • Anatomic delineation of occlusion and collaterals • Plan operative revascularization • Allow infusion of therapeutic agents (lytics, vasodilators) 1 Ann Surg 2001;233(6):801-808
Principles of Treatment • Diagnose • Restore Flow • Resect non-viable tissue • Supportive Care • Second-Look
Therapy Supportive measures • IV resuscitation • Optimize cardiac status • Broad-spectrum antibiotics (no data) • Nasogastric decompression
Therapy: Pharmacologic Anticoagulation • Heparin IV • Prevents clot propagation • Systemic vs. intra-arterial • Timing of initiation • Immediately vs. 48 hr delay1,2 • Restart 48 hrs after surgical intervention • Warfarin • Prevents clot propagation • Give for 6-12 mos if no clotting disorder (no data) 1 Surg Gynecol Obstet 1981;153:561-569 2 Vascular Emergencies. 1982;553-561
Therapy: Pharmacologic Vasodilators • Papaverine (30-60 mg/hr) • Increases cAMP, relaxes smooth muscle • Primary indication: Non-occlusive arterial disease • Criterion for use: • Peritoneal signs absent • Cannot undergo surgery • Must have good distal perfusion bed
Therapy: Pharmacologic Vasodilators (cont.) • Papaverine • Early SMA infusion reduces mortality to 40-50%1 • Directed infusion via angiography • Rx: 24-48 hrs • Endpoints both clinical and angiographic • Subsequent surgery 1 Surg 1977;82:848-855
Therapy: Pharmacologic Thrombolysis • urokinase>streptokinase, rtPA • Short t½, easily reversed • Dose: high vs. low • 5,000 U/hr - 600,000 U/hr • Direct SMA infusion vs. operative placement Am Surg 2004;70(7):600-604
Therapy: Pharmacologic Thrombolysis • Duration: minutes – 48 hrs1 • too long → risk of bowel necrosis • Treat to re-establish flow vs. complete dissolution • > 48 hrs • Greater risk of bleeding • Discontinue • Worsening abdominal symptoms without evidence of thrombolysis • Bleeding • No angiographic improvement 1 JVIR 2005;16:317-329
Pooled Data JVIR 2005;16:317-329
Outcomes • Technical success: 43/48 • Technical failure: 5/48 • Outcome most dependent on age of thrombus/embolus • Improvement of abd pain in 1st hour is a favorable prognostic sign • Technical success does not equal clinical success • Survival: 43/48 • Safety JVIR 2005;16:317-329
Therapy: Pharmacologic Thrombolysis • Criterion for use: • Embolic/thrombotic disease • Poor operative candidates • No contraindications to fibrinolytics • No bowel infarction (no peritonitis/acidosis) • Expansion of use to all patients without bowel infarction
Therapy: Endovascular Angioplasty/Stenting • Long-term durability questioned vs. surgical repair • Utility in acute ischemia setting • Advantages: • Shorter duration of treatment than thrombolysis • Definitive treatment JVIR 1999;10(7):861-867
Therapy: Endovascular Angioplasty/Stenting • Ideal for thrombotic lesions • Calcified ostial lesions • Flow-limiting dissections • Chronic occlusion • Advanced techniques for embolic lesions • Flow-limiting dissections • Embolectomy w/distal protection
Therapy: Endovascular J Vasc Surg 2003;38:692-8
Therapy: Endovascular Stenting Outcomes (Chronic, SMA/Celiac) 1998: Primary patency 100% at 14 mos (n=3)1 0% mortality 1999: Primary patency 74% at 18 mos (n=12)2 8.3% mortality <30 days 2003: Technical success 96% (n=26)3 Clinical success 88% Primary patency at 34 mos 65% Restenosis at 34 mos 12% 1 Cardiovasc Int Radiol 1998;21:305-313 2 JVIR 1999;10(7):861-867 3 J Vasc Surg 2003;38:692-8I
Therapy: Endovascular Stenting Indications • Simple stenotic lesions • Complex lesions (long-segment, irregular, heavily calcified) • Total occlusion Contraindications • Suspected bowel necrosis (peritonitis, acidosis, etc) • diffuse distal disease • Median arcuate ligament compression syndrome 1 J Vasc Surg 2003;38(4):692-8
Surgery Anyone with peritonitis needs to be explored. • Midline incision • Evaluate extent of ischemia • Doppler of entire SMA • Revascularization (embolectomy vs. bypass) • Re-evaluate ischemia • Lastly, non-viable bowel must be resected
Surgery:Options for Revascularization Ann Vasc Surg 2003;17:72-79
If embolus suspected, transverse arteriotomy proximal to middle colic takeoff Embolectomy Allow reperfusion for 20-30 minutes and then re-assess bowel viability Surgery:Principles Curr Opin Cardiol 1999;14(5):453-460
Thrombosis requires a bypass Longitudinal arteriotomy Thrombectomy Inflow adequate: Inflow inadequate: Bypass Vein vs. graft Surgery:Options for Revascularization Curr Opin Cardiol 1999;14(5):453-460
Surgery:Options for Revascularization Curr Opin Cardiol 1999;14(5):453-460
24-hr second look operation Ischemia continues after acute event and reperfusion No way to determine viability initially Allows time for supportive measures to recover tissue Surgery:Damage Control