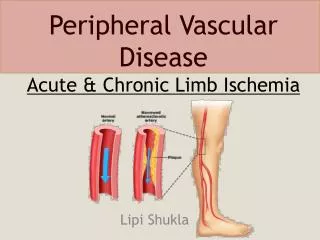
Acute Mesenteric Ischemia
Acute Mesenteric Ischemia. Scott Q. Nguyen, M.D. Celia M. Divino, M.D. Mount Sinai School of Medicine Department of Surgery. Mrs. Mitty. An 83 year-old woman is brought to the ER by ambulance from her nursing home w/ a 4 hour history of severe diffuse abdominal pain and distention . History.

Acute Mesenteric Ischemia
E N D
Presentation Transcript
Acute Mesenteric Ischemia Scott Q. Nguyen, M.D. Celia M. Divino, M.D. Mount Sinai School of Medicine Department of Surgery
Mrs. Mitty An 83 year-old woman is brought to the ER by ambulance from her nursing home w/ a 4 hour history of severe diffuse abdominal pain and distention.
History What other points of the history do you want to know?
History, Mrs. Mitty Characterization of symptoms Temporal sequence Alleviating / Exacerbating factors: Pertinent PMH, ROS, MEDS. Associated signs and symptoms Relevant family hx. Consider the Following
History, Mrs. Mitty Characterization of Symptoms: Sudden onset diffuse abdominal pain and distention 4 hours ago. Pain not localized to any quadrant. Alleviating / Exacerbating factors: Pain is excruciating, it’s the worse she’s ever experienced Nothing alleviates it Associated signs/symptoms: She vomits 1L of feculent emesis on arrival to ER. Last BM 2 hours ago, loose
Other History PMH Atrial Fibrillation - dx’d 1 month ago, anticoagulation contraindicated with history of massive GI bleed CHF, CAD, DM PSH Cholecystectomy, left hemicolectomy for diverticular disease MEDS digoxin, metoprolol, insulin
Other History Social History Occasional wine, 50 pack-yr smoker, quit 2 yrs ago Family History Patient unable to give
Differential DiagnosisBased on History and Presentation Small Bowel Obstruction Acute Mesenteric Ischemia Perforated Diverticulitis Ischemic Colitis Perforated Peptic Ulcer Disease Acute Pancreatitis Acute Cholecystitis Gastroenteritis Acute Appendicitis
Physical Examination What would you look for?
Physical Examination Vital Signs: T = 38.5, P = 103, BP = 140/85, RR = 28 Appearance: thin , in severe distress, legs pulled up to chest, moaning Heart: irregularly irregular Lungs: mild rales at bases Abdomen: decreased BS, very distended, mildly tender diffusely, no guarding/rebound tenderness, no hernias Rectal: loose stool in vault, streaked w/ fresh blood Remaining Examination findings non-contributory
Laboratory What would you obtain?
LFTs - WNL Amylase/Lipase - 89/95 PT/PTT - 13.0/33.0 ABG - 7.31/30/69/16 Lactate 7.9 Labs ordered, Mrs. Mitty 14 30 133 101 405 18 240 42 1.2 4.9 19 85 PMN’s 22 Bands
Lab Results, Discussion Leukocytosis - acute process, possibly infectious Electrolytes - elevated BUN indicating dehydration or 3rd spacing. Anion gap acidosis - intravascular depletion, Metabolic acidosis (lactic acidosis) Coags –abnormal coags may reflect sepsis. Pt. not on anticoagulation for Afib. Normal LFTs/ pancreatic enzymes - no signs of hepatic/pancreatic insult
Consider the following Interventions Admit to the hospital/ICU Aggressive resuscitation Start IV with isotonic crystalloid solution ( NS or LR) Insert Foley catheter Monitor response to resuscitation Administer broad spectrum antibiotics Likely intra-abdominal septic process
Studies What further studies would you want at this time?
Studies, Mrs. Mitty Abdominal X-rays Flat / Upright Acute Abdominal Series (may include chest at some institutions)
Studies – Results Plain abdominal films Diffuse dilation of small bowel w/ air fluid levels on upright view. Some air in Left colon and Rectum. NO free air
Revised Differential Diagnosis Acute Mesenteric Ischemia Strangulated small bowel obstruction Diverticulitis w/ contained perforation?
What next? Mesenteric Angiogram or CT Angiogram
Discussion With the sudden onset of symptoms, h/o Afib, and “pain out of proportion to physical exam,” acute mesenteric ischemia should be high on the Differential Diagnosis A mesenteric angiogram will allow visualization of the visceral vessels (celiac, SMA, IMA)
Mesenteric Angiogram Note complete lack of contrast in mesenteric vessels in AP view (left). The occluded origins of the celiac axis and superior mesenteric artery are demonstrated in the Lateral view (right).
CT Angiogram Note complete occlusion and lack of IV contrast filling the superior mesenteric artery from its origin from the aorta (Arrows).
Other studies CT angiogram / MR angiogram sensitivity 75%, specificity 100% for emboli additionally can detect thickened, distended bowel loops more sensitive for Mesenteric Venous Thrombosis
Management What should be done next?
Management Pre-operative preparation Assure adequate resuscitation Monitoring Foley Catheter Urgent exploration Surgical embolectomy Assess bowel viability
Management Pre-operative preparation Assure adequate resuscitation Monitoring Non-invasive: EKG, BP, Pulse Oximetry, foley catheter Consider invasive monitoring: Central venous catheter, PA Catheter ? Arterial line? Operative Technique/ Urgent exploration Midline Laparotomy Relevant Anatomy Surgical Embolectomy Assess bowel viability
Surgical Embolectomy Pack bowel to Right, Expose SMA Arteriotomy Pass balloon embolectomy catheter Assess bowel viability Resect if necessary Necrotic bowel from mesenteric ischemia.
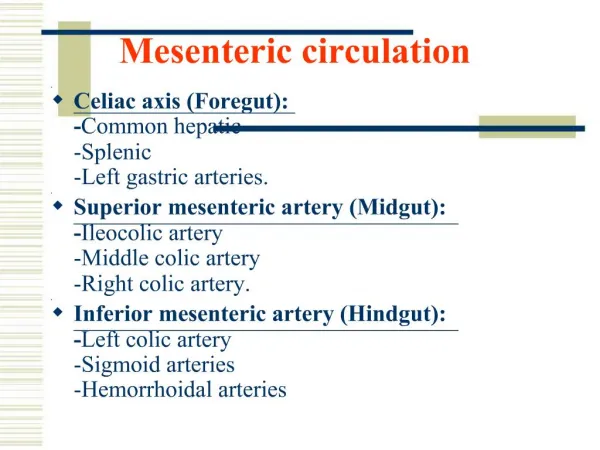
Discussion Acute mesenteric ischemia is a vascular emergency with overall mortality 60-80%. There are four main pathophysiologic processes which have the same common endpoint, bowel necrosis, abdominal sepsis, and death. Mesenteric arterial anatomy is notable for rich collateral flow between the celiac trunk, superior mesenteric artery, and inferior mesenteric artery. Gradual occlusion of 2 of the 3 vessels is tolerable as rich collateral branches form between these. Acute occlusion of any of the vessels or their branches causes acute intestinal ischemia and necrosis.
Discussion The four processes: 1) Acute arterial embolus -usually from cardiogenic embolus in pts w/ Afib or valvular disorders. SMA is the common vessel affected as it has a less acute take off from aorta 2) Acute arterial thrombosis - chronic atherosclerotic plaque at origin of vessel acutely thromboses 3) Chronic mesenteric ischemia - atherosclerosis of visceral vessels results in abdominal pain (intestinal angina) during times of increased blood demand (digestion) Acute venous occlusion - venous thrombosis causes cessation of venous outflow from intestines *Non-occlusive mesenteric ischemia can also be seen in low-flow states
Discussion Diagnosis- requires high degree of suspicion. Classically presents as “pain out of proportion to physical exam” or severe pain w/o peritoneal signs. The history of Cardiac disease, valvular disease, or Afib should alert one to an embolic disease. Gold standard for diagnosis is mesenteric angiogram, but CT angiogram is more and more being used. Treatment - requires aggressive resuscitation and hemodynamic monitoring as patients become critically ill very quickly. Urgent surgery w/ viseral revascularization (embolectomy, thrombectomy, endarterectomy, or bypass) is required. After this, evaluation of viability of bowel segments should be performed with resection of any necrotic portions.
References Townsend CM. Sabiston Textbook of Surgery. 17th Edition Cameron JL. Current Surgical Therapy. 8th Edition Oldenburg et al. Acute Mesenteric Ischemia. Arch Intern Med 164:1054-62. 2004
Acknowledgment The preceding educational materials were made available through theASSOCIATION FOR SURGICAL EDUCATION In order to improve our educational materials wewelcome your comments/ suggestions at: feedbackPPTM@surgicaleducation.com