Download
1 / 33
440 likes | 1.19k Vues
Endovascular Treatment for Acute Limb Ischemia. M Mazen Hachem *, MD, PhD, FACS., M Bosaeed * and M Wakka * Gh . Atasi **, A. Qanawi **, M Brembali **, *Division of Vascular Surgery **Division of Interventional Radiology King Abdul-Aziz Medical City Jeddah, KSA. Introduction.

E N D
Endovascular Treatment for Acute Limb Ischemia • M MazenHachem*, MD, PhD, FACS.,M Bosaeed* and M Wakka* • Gh. Atasi**, A. Qanawi**, M Brembali**, • *Division of Vascular Surgery • **Division of Interventional Radiology • King Abdul-Aziz Medical City • Jeddah, KSA
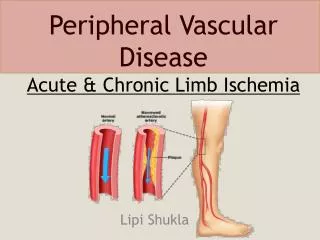
Introduction • Acute Limb Ischemia is a catastrophic event • Threatens both the patient's limb and life. • Traditionally, Surgery has been the “gold standard” • However, the multiplicity and complexity of medical co morbidities • Account for high rates of perioperative morbidity and mortality. • Blaisdell’s landmark study (1978) • Death in 30% of patients, amputation in 25% of survivors
Introduction • These results have prompted interest in a less invasive treatment strategy for ALI. • In recent years, Catheter-Directed Thrombolysis Therapy (CDT) became the treatment of choice for many patients in acute limb ischemia. Thrombolysis in the Management of Lower Limb Peripheral Arterial Occlusion—A Consensus Document J VascIntervRadiol 2003; 7:S337–S349
Aim • To assess the efficacy & safty of CDT in patients with ALI and semi ALI • Initial success rate • M & M rates of CDT will be discussed.
Methods:Patients • Inclusion Criteria • Category I, IIa, IIb • Clinical Category of SVS/ ISCSV • Catheter penetrate the thrombotic or embolic occlusion • Exclusion criteria • Limb-threatening ischemiarequiring immediate surgery • Non penetrable occlusion • Contraindication of thrombolysis
Clinical Categories of ALI SVS/ ISCVSII Venous Doppler Signals Arterial Doppler Signals Description or Prognosis Sensory Loss Muscle Weakness Category II. Viable II. Threatened a. Marginally b. Immediately III . Irreversible None Minimal (toes) or none More than toes; associated with rest pain Profound, anesthetic None None Mild to moderate Profound paralysis (rigor) Audible (Often) inaudible (Usually) inaudible Inaudible Audible Audible Audible Inaudible Not immediately threatened Salvageable ifpromptly treated Salvageable with immediate revascularization Major tissue loss or permanent nerve damage inevitable Rutherford et al. J Vasc Surg. 1997;26:517–538.
Methods: Protocol & Procedure • rtPA was administrated through a coaxial catheter, multi-holes impeded in the thrombus • 5X5X5 mg in 15min interval as bolus (pulse spray technique) • Control angio. 1/h + readjustment of cath. • 0.5-2mg rtPA/ h by infusion pump. • Heparin 500-1000U/h through vascular sheath side port. (APTT ratio 1.5-2). • ICU setting
Methods:Protocol & Procedure • Clinical/Angiographic evaluation • CDT termination • Worsening or no clinical improvement in 2h • Complications required its cessation • Adequate vessel patency was achieved
Methods:Protocol & Procedure • Success was defined as: • Clot lysis sufficient to restore anterogradeflow throughout the previously occluded segment. • Clinical improvement even with moderate angiographic success • Complementary PTA when indicated.
Results: Patient Characteristics • Thirty tow patients • M/ F ratio: 1.7 • Median age 64 years • 78% were diabetics. • 33 limb (7 upper limbs, 26 lower limb) • 30 limbs (82%) were classified as category I, IIa • 3 limbs (9%) were IIb • 3 limbs (9%) were IIIa • Underwent CDT at our institution from December 2003 to June 2008.
Results: Patient Characteristics • The underlying causes of ALI • 48.5% arterial thrombosis • 35.5% arterial embolism • 18% graft occlusion • Ischemia duration • 70% < 14 days
Results: Patient Characteristics • The arterial sectors involved • Femoral in 12 cases • Popliteal in 4 cases • Aortoiliac in 1 case • Distal in three cases • Subclavian in 5 cases and brachial in tow • Aorto-bi-femoral bypass in one. • Fem-Distal PTFE bypass in 2 • Fem-Distal venous bypass in 2
Results • All had CDT, some followed by PTA. • Except • 7 /11 embolectomy with distal peroperative CDT • 2 redo bypasses (PTFE) with distal peroperative CDT
Results • rtPA dose range 30 to 100mg • Mean duration 18h (range: 12 to 60h)
Results: Outcome • 91% limb salvage. • 10% had recurrence in one month • 6% major limb amputations • One below knee • One below elbow • 3% hospital mortality • 12.5% had bleeding around the catheter • In tow patients CDT were stopped • Saved limbs
Discussion • Even our patients are: • Heterogeneous, encompassing occlusionof grafts and native arteries • Thrombotic and of embolicorigins • Upper and lower extremities • < > 14 days of limb ischemia • 78% diabetics
Discussion • CDT induced recanalization in 91% • Within a mean of 18 hours (range,12to 60 hours). • The rtPA protocol followed was as recommended by Eu. Consensus 2003. • The last 12 patients 0.5 mg rtPA/h was used • No difference was found between high and low dose. • Duration • Bleeding
Duration of occlusion Location Thrombosis/embolism Motor loss Age/sex Diabetes status Wire passage Catheter in clot Conduit material No.: Segment involved Predictors of Success: CDT Insignificant Variables Significant Variables Ouriel et al. Radiology. 1994;193:561–566.
Statistically Significant Predictors of Successas Determined by Multivariate Analysis Odds Ratio (95% CI) P Value Variable Medical history of diabetes Procedure Catheter into thrombus Guide wire traversal of thrombus Segments involved* One Two Conduit type Native artery Prosthetic grafts 0.75 (0.40—0.89) .044 7.40 (2.11—16.90) .001 3.10 (1.72—8.52) .003 1.60 (1.47—1.79) .0151.42 (1.29—1.77) .029 1.25 (1.05—1.42) .0411.51 (1.11—1.92) .017 *Grafts were counted as one segment. Ouriel et al. Radiology. 1994;193:561–566.
Guide wire traversal Guidewire
Popliteal Thrombosis Initial Angio Thrombolysis Final Result
CDT & PTA Initial Angio Thrombolysis PTA Final Result
Comparing Surgery and Lysis: What Data Exist? • The Rochester Trial:1994, 114 patients, UK vsOperation 2. The STILE Trial: 1994, 393 patients, rt-PA vs UK vsOperation 3. The TOPAS Trial: Phase I: 1996, 213 patients, r-UK dose range Phase II: 1998, 544 patients, r-UK vs Operation
The Rochester Trial1-Year Data Incidence of Clinical Events (%)
The STILE Trial: 1-Month Data Incidence of Clinical Events (%) The STILE Trial. Ann of Surg. 1994;3:251–268.
Heparin + CDT • Therapeutic heparinization with thrombolysis has been controversial: • Most clinicians used systemic heparinization 500 U/hr) in conjunction with thrombolysis. Blaisdell’s landmark study (1978
Discussion • Our data showed • No amputation in category IIb • Long ischemic duration in IIa resulted in limb salvage. • Severe bleeding in 2 patients could not be attributed to heparin 500U/h, PTT ratio: 1.5 • Our death was not related to CDT • Saved limb • M & M were from IIIa
Conclusion • CDT has been shown to be safe and useful for rapid release of ischemic symptoms by clot dissolution /Complete or partial • CDT has low rates of morbidity and mortality. • CDT unmasking underlying stenoses, • Helping to determine the best treatment strategy in elective basis • PTA • Surgery.