PLEURAL EMPYEMA
PLEURAL EMPYEMA. Department of Thoracic, General and Oncological Surgery Medical University of Lodz Head of the Department: Prof. Marian Brocki. Author of the lecture: Sławomir Jabłoński, MD. DEFINITION. Pleural empyema. or. thoracic empyema. The inflamatory process in a preformed

PLEURAL EMPYEMA
E N D
Presentation Transcript
PLEURAL EMPYEMA Department of Thoracic, General and Oncological SurgeryMedical University of Lodz Head of the Department: Prof. Marian Brocki Author of the lecture: Sławomir Jabłoński, MD
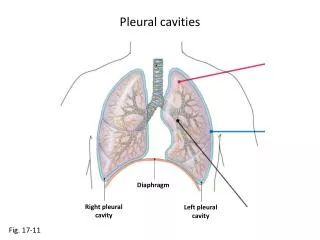
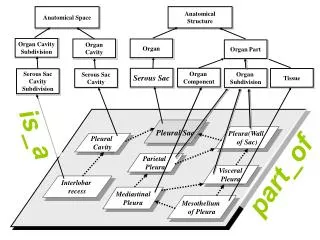
DEFINITION Pleural empyema or thoracic empyema The inflamatory process in a preformed anatomical space defined by the visceral and parietal pleura
Incidence & epidemiology • Empyema is the presence of gross pus in the pleural cavity; it consists of an effusion containing polymorphonuclear leukocytes and fibrin. • The Greek philosopher, Aristotle, recognized empyema and described the drainage of pus with incision and a metal tube as early as 300 BC. • A parapneumonic process is defined as a pleural effusion associated with pneumonia, lung abscess or bronchiectasis. • Not all parapneumonic processes are empyemas.
PLEURAL EMPYEMA (empyema pleurae) Pleural empyema is a kind of exudative pleuritis caused by microorganisms (bacteria, fungi, some protozoa) that infected the pleural cavity. Inflammation of organs or anatomical structures localized within the chest and out its anatomical borders can caused a retention of effusion in thepleural space (hydrothorax) A reason for pleural effusions are also systemic diseases. Initially sterileexudate can be resorbed by the pleura if a primary disease is treated effectively. The infection of the exudate causes its transformation into purulent liquid that fills the pleural cavity and forms pleural empyema (empyema pleurae).
PLEURAL EMPYEMA (empyema pleurae) The presence of purulent liquid within the pleural cavity for several Weeksleads to the formation of fibrin deposits on both the visceral and parietal pleuraand an imprisoning fibrothorax appears (fibrothorax). Progressing empyema organization causes lung compression and atelectasis,decreases lung volume and leads to inflammatory changes within pulmonary parenchyma. As a result ventilation and gas exchange disturbances are observed. Within a fibrinopurulent capsule (membrana pyogenes) a collection of pus is frequently present. However, septic liquid has no contact with adjacent tissuewell supplied with blood that’s why a clinical presentation of empyema may be uncharacteristic and poorly expressed.
PLEURAL EMPYEMA (empyema pleurae) • CLINICAL CONDITIONS CAUSING LIQUID RETENTION IN THE PLEURAL CAVITY : • TRANSUDATE -circulatory insufficiency, hepatic cirrhosis, nephrotic syndrome, superior vena caval obstruction. • EXUDATE – malignancy, infection, pulmonary embolism, esophageal perforation, pancreatitis, sarcoidosis, systemic diseases. • LYMPH (chylothorax) – trauma, surgery, malignancy, subclavian vein thrombosis. • BLOOD (haemothorax) - trauma, malignancy In a case when a liquid collected in the pleural space becomes infected by virulent microorganisms it transforms into pus. Pleural empyema can develop in any individual but it seems to be more frequent in younger people in whom immune system is weakened.
PLEURAL EMPYEMA (empyema pleurae) The most frequent reason for pleural empyema are complications of pneumonia (parapneumonic empyemas) and other diseases of tissues adjacent to the pleural cavity. An important etiological group for pleural empyema are complications of surgical treatment of pulmonary, esophageal and mediastinal pathologiesand frequent, repeated thoracocentesis for pleural effusion. Lung resections with incomplete postoperative expansion of the lung promote the formation of a cavity that creates good conditions for liquid retention and its infection with bacteria from the bronchial tree, infected postoperative wound or drains. Complications of thoracic injuries and among them the infection of non-evacuated posttraumatic hemothorax are significant etiological factors of pleural empyema formation.
PLEURAL EMPYEMA (empyema pleurae) • MICROBILOGY - BACTERIOLOGIC AGENTS: • Most common bacteriologic agents : • pneumococus • staphylococus • streptococus • haemophilus influenzae • Gram-negative bacteria (pseudomonas, klebsiella, enterobacteriace,escherichia coli) • anaerobic bacteria • mixed bacterial flora
PLEURAL EMPYEMA (empyema pleurae) • PATHOPHYSIOLOGY – ways of infection : • DIRECT INFECTION through the chest wall as a result of injury, thoracocentesis or surgical management (postoperative pleural empyemas constitute approximately 25% of pleural empyema cases) • CONTACT INFECTION – infection spreads from underlying infected pulmonary parenchyma, lung abscess, bronchiectases, subphrenic or perinephric abscess. • HEMATOGENOUS SPREAD • LYMPHOGENOUS SPREAD
PLEURAL EMPYEMA (empyema pleurae) • PATHOPHYSIOLOGY PHASES OF PLEURAL EMPYEMA FORMATION : • Serous phase (exudative empyema): clear, straw-colored effusion (pH>7.3, glucose concentration [GLU]>60 mg%, lactate dehydrogenase activity[LDH] < 500 U/L ) • Fibrinopurulent phase (fibrinopurulent empyema): effusion contains large numbers of bacteria and polymorphonuclear granulocytes, intensification of clinical signs and symptoms of inflammation, deposition of fibrin on both the visceral and parietal pleura ( pH < 7,1, GLU < 40mg%, LDH > 1000 U/L) • Organizing empyema phase (organizing empyema)(fibrothorax) – nonelastic, fibrinopurulent coat that imprisons the lung appears. An empyema capsule contains pus.
PLEURAL EMPYEMA (empyema pleurae) • CLASSIFICATION OF PLEURAL EMPYEMAS : • Etiological classification: • specific (tuberculosis) • non-specific – non-specific bacterial infection • mixed • mycotic Pathogenetic classification: • synpneumonic – empyema coexists with another lung inflammation • metapneumonic – it develops when a primary inflammation has already regressed
PLEURAL EMPYEMA (empyema pleurae) • CLASSIFICATION OF PLEURAL EMPYEMAS : • Size criterion: • non-localized empyemas – the whole pleural cavity is involved • localized (encapsulated) empyemas - ( unilocular or multilocular) Duration and pathologic criterion : • acute empyema • chronic empyema Jatrogenic empyemas: • empyemas with preserved pulmonary parenchyma • empyemas after lung resection (pneumonectomy) • with bronchial fistula • without bronchial fistula
PLEURAL EMPYEMA (empyema pleurae) CLINICAL PRESENTATION: • ACUTE PHASE: • hectic fever • shivering • dyspnea • toxemia • chest pain • tachypnoë • asthenia • lack of appetite • weight loss • chest wall inflammation (sometimes) • leucocytosis • anemia • expectoration of purulent sputum ( if bronchial fistula coexists) • CHRONIC PHASE: • subfebrile body temperature • cachexia • low body mass • paroxysmal cough • dyspnea • contraction of intercostal spaces • scoliosis • chest pain • attenuation of respiratory murmur • dullness of sound
PLURAL EMPYEMA (empyema pleurae) • DIAGNOSIS : • characteristic clinical presentation • features of hydrothorax in physical examination • chest X-ray • pleural ultrasonography • computed tomography • diagnostic thoracocentesis( macroscopic features of liquid, positive bacterial cultures, glucose concentration< 40 mg/dl, pH<7,0, LDH > 1000 U/L) • flexible bronchoscopy (useful in a case of bronchial fistula) • needle pleural biopsy • diagnostic videothoracoscopy • diagnostic thoracotomy
PLEURAL EMPYEMA (empyema pleurae) • ROENTGENOGRAPHIC APPEARANCE OF PLEURAL EMPYEMA : • opacification of the costophrenic angle compatible with pleural effusion (the beginning of the disease) • roentgenographic features of lung compression caused by effusion (Ellis-Damoiseau line) • the presence of an empyema capsule, on a lateral projection empyema has a D-like shape. • the mediastinum is shifted to the contralateral side of the chest • pneumothorax with airfluid level (if bronchial fistula is present) • roentgenographic features of empyema and spherical opacification within pulmonary parenchyma (empyema accompanied by lung abscess)
LUNG EMPYEMA (empyema pleurae) TREATMENT : The treatment of pleural empyema depends on its etiology, duration, patient’s general state and concomitant diseases. The general rules of empyema management are as follows: evacuation of purulent liquid out of the pleural space, obliteration of the empyema sac and augmentation of patient’s immune system. Ubi pus evacua - ,,if you find pus remove it” • The goals of treatment in pateints with pleural empyema are : • to save life • to elimintae the empyema • to reexpand the trapped lung • to restore the mobility of the chest wall and diaphragm • to return respiratory functionto normal • to eliminate complications and chronicity • to reduce the duration of hospital stay • (Mayo P, Saha SP, McElvein RB. Acute empyema in children treated • by open thoracotomy and decortication. Ann Thorac Surg. 1982;34:401-407)
TREATMENT : • ACUTE EXUDATIVE EMPYEMA : • exudative empyema can be treated by aimed antibiotic therapy and repeated needle aspirations of pleural effusion. • simultaneously coexistent pathologies are treated and nutritional therapyis carried out. • intercostal tube drainage is usually a primary treatment for both acute and chronic pleural empyema. • intrapleural antibiotic administration
PLEURAL EMPYEMA (empyema pleurae) • TREATMENT : • CHRONIC EMPYEMA : • suctionintercostal tube drainage with interpleural antibiotic administration • irrigating pleural drainage • after 14 days a suction drainage can changed into an open drainage and a patient can continue his or her therapy in an outpatient clinic. • interpleural administration of fibrinolytic agents in a case of encapsulated empyema (Streptokinase or Streptodornase for 3-5 days) • videothoracoscopy with mechanical debridement of the pleural space , ablation of dividing walls within the empyema, partial decortication and pleural drainage.
PLEURAL EMPYEMA (empyema pleurae) • SURGICAL MANAGEMENT : • thoracotomyand decortication- if by intercostal tube drainage lung re-expansion isn’t achieved (decortication- a nonelastic fibrinopurulent coat is removed from the underlying lung and the chest wall to make re-expansion of the lung possible) • decortication and lung resection ( empyema is accompanied by lung abscesses, lung mycosis or malignancy) • chest wall fenestration- a technique used in debilitated patients. An upside down U-shaped skin incision is made to form a musculocutaneous flap. Short fragments of 2 or 3 ribs are resected over the most dependent part of the empyema sac. Then the flap (Eloesser flap) is introduced into the pleural space and sutured together with the parietal pleura. A kind of a channel is formed that enables effective pus drainage and repeated introduction of gauze saturated with antiseptic agents. Such a management leads to gradual sterilization of the pleural space and its healing by granulation.
SURGICAL MANAGEMENT: • in patients with pleural empyema after lung resection the ablation of the empyema sac by a surgical reduction of its size is the main goal (thoracoplasty, myoplasty, omentoplasty). • in patients with pleural empyema with bronchial fistula after pneumonectomy - removal of the empyema sac (membrana pyogenes) and the closure of the fistula (myoplastic procedures- bronchial fistula is covered with a pedunculated muscle bundle) plus thoracoplasty. • Clagett procedure - chest wall is fenestrated. When the healing of the parietal pleura by granulation appears the fenestration is closed and the pleural space is sterilized by its filling throughout a drain with a solution of antibiotics selected on the basis of bacterial cultures • Weder procedure- three successive thoracotomies are performed every 2-3 days. During the first and the second thoracotomy fibrinopurulent empyema sac is removed and gauze saturated with antibiotic solution is placed within the pleural space. During the third thoracotomy gauze is removed.
Treatment of pleura empyeme Thoracocentesis Clear liquid Not clear or purulent effusion pH>7.20 pH<7.20 Not loculated Loculated No intervention Reccurent thoracocentesis Drainage Pleural lavage Drainage Pleural lavage Fibrinolytics Failure VATS Surgery Hamm et al, ERJ 1997
MYOPLASTY in treatment of bronchial fistula post pneumonectomy
Post lung resection empyema Post lobctomy(0,01%-2,0%), post pneumonectomy (2%-16%), residual space and air leak Methods of tretment: - Muscle flap clousure - Limited thoracoplasty - Open window thoracostomy
The Clagett procedure -open-window thoracostomy in patient with pleural empyema and bronchial postpneumonectomy fistula (own meterial)
PLEURAL EMPYEMA (empyema pleurae) • EMPYEMA COMPLICATIONS : • atelectasis and respiratory insufficiency • bronchopleural fistula • pleurocutaneous fistula • pleuroesophageal fistula • sepsis • peritonitis • metastatic abscesses • purulent inflammation of the chest wall • progressive respiratory insufficiency
PLEURAL EMPYEMA (empyema pleurae) PROGNOSIS : Mortality in patients with pleural empyema ranges from 1% to 19%. A reason for death in an acute phase of empyema is sepsis or other complications of generalized infection. Late deaths are caused by toxemia, respiratory insufficiency or multiorgan failure. In patients with concomitant diseases such as diabetes mellitus, malnutrition, systemic diseases, malignancy and alcoholism mortality reaches 40%.