
Muscle Hydration Assessment in ESRD Patients on Hemodialysis: cBIS vs. MRI
This study explores the relationship between calf bioelectrical impedance spectroscopy (cBIS) and MRI-acquired measures to evaluate muscle hydration in people with end-stage renal disease (ESRD) undergoing hemodialysis. The aim is to assess the impact of fluctuating hydration levels on muscle function, particularly focusing on the tibialis anterior muscle. The study also investigates the association of cBIS ECF with MRI T2 values of leg muscles and apparent diffusion coefficient (ADC) to estimate muscle hydration levels accurately. Key findings will help understand the importance of muscle hydration in ESRD patients and its implications for muscle health and overall well-being.

Muscle Hydration Assessment in ESRD Patients on Hemodialysis: cBIS vs. MRI
E N D
Presentation Transcript
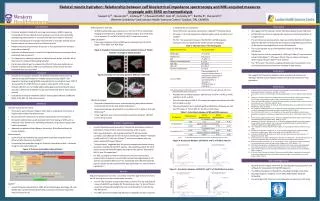
Skeletal muscle hydration: Relationship between calf bioelectrical impedance spectroscopy and MRI-acquired measures in people with ESRD on haemodialysisSawant A1,2, House AA1,2, Lindsay R1,2, Chesworth BM1, Gati JS1, Connelly D1,2, Bartha R1, Overend TJ1Western University1 and London Health Sciences Center,2 London, ON, CANADA Introduction Discussion • Particular problems linked with end-stage renal disease (ESRD ) requiring hemodialysis (HD) are skeletal muscle weakness and renal osteo-dystrophy, predisposing these patients to increased fall rates and long bone fractures1 • Exercise training has been strongly recommended to maintain skeletal muscle function and as such prevent falls and related injuries2 • However the presumed benefits of exercise in this population have not been observed consistently3 • Hydration of skeletal muscle is one of the important factors for adequate force production and endurance4 • It is important to establish hydration of skeletal muscle before and after HD to determine the impact of fluctuating hydration • Our primary interest was to evaluate the effect of fluctuating hydrations on function of tibialis anterior (TA) since insufficiency of this muscle has been associated with increased falls5 • Evaluate the association between extracellular fluid (ECF) of the lower leg measured using calf bioelectrical impedance spectroscopy (cBIS)6,7and magnetic resonance imaging (MRI) acquired transverse relaxation times (T2)8 of TA to establish if calf BIS ECF can be used to estimate ECF of TA muscle • Evaluate cBISECF vs T2 of medial (MG), lateral gastrocnemius (LG) and soleus muscles to determine if cBIS ECF can be used to estimate ECF of these specific muscles • Evaluate the association between cBIS ECF and apparent diffusion coefficient (ADC) of TA, MG, LG, and soleus muscles Inclusion and exclusion criteria: • Participants were 18 years of age or older, able to understand instructions in English and provided informed consent • No documented evidence of any disease impacting the nervous systems • No health condition that would preclude them from having an MRI, such as aneurysm clips, dental work, indwelling stimulators, drug infusion pumps and cardiac pacemaker • Approval was obtained from Western University’s Ethics Review Board for Human Subjects Questionnaires: • Levels of self-reported physical activity were quantified using the Human Activity Profile Questionnaire (HAP)10 • Comorbidity was quantified using the Charlson Comorbidity Index11calculated using the automated calculator Figure 1: Charlson comorbidity index calculator Calf ECF • A multi-frequency device (Xitron 4200, Xitron Technologies, San Diego, CA, USA 92126) was used for estimating ECF using automatic continuous sequential measurements of calf MRI acquired T2 and ADC • All MRI-acquired data was collected on a 3.0 Tesla Tim Trio whole body imaging system (Siemens, Erlangen, Germany) using an 8-channel knee coil to measure T2 and ADC of the TA, MG, LG and soleus muscle Data Calculation: • Transverse relaxation times and ADC were calculated using the OsiriX plugin "T2 Fit Map" and “ADC Map” Figure 2: Example of measuring transverse relaxation times of Tibialis Anterior: T2 Image of Tibialis Anterior Figure 3: Example of measuring apparent diffusion coefficient Statistical Analysis: • Participant characteristics were summarized using descriptive statistics and presented as means and standard deviations • Required sample was calculated for a correlation of 0.5, alpha of 0.05 and 80% power12 • Linear regression was used to determine association between cBIS ECF and T2 of leg muscles • A priori hypotheses were grounded in theoretical assumptions based on distribution of type II fibers and the size/volume of the muscles • Fiber-type distribution : Wehypothesized that T2 will have better correlation with cBIS ECF for the TA muscle (~50% type II fibers)13 followed by MG and/or LG (~43% type II fibers)14 and least correlation with the soleus muscle (20% type II fibers)14 • “Volume theory” suggested that the muscle occupying maximum volume would also include the most ECF volume.We hypothesized that the T2 of soleus muscle will have the highest correlation with cBIS ECF followed by MG, LG and TA respectively15 • For ADC, as people on HD are known to have reduced muscle mass, reduced ratio of capillary to muscle fiber and perhaps degradation of cell wall due to substrate deficiency15 the relationship with cBIS ECF would be poor for all the muscles based on fiber type distribution or volume theory hypothesis 16 Required sample of 22 (11 men, 11 women) volunteers (age: 50.6 ±15.7 years) on HD meeting the inclusion criteria were recruited • For the cBISECF data, one participant was an outlier. The pre and post HD values of cBIS ECF were higher for this participant; had ~ 6 liters of fluid in excess of estimated dry weight that was not dialyzed to it’s nadir during the HD session • The HAP scores for the MAS and AAS were comparable to those reported in literature for this population • These HAP scores have been classified as “impaired”6functional levels. • CCI index > 3.0 in this population indicated higher risk of mortality in this sample17 • Pre HD – the association between the cBIS ECF and MRI acquired measures were not significant for all the muscles investigated Table 1: Characteristics of the Participants AAS: adjusted activity score, BMI: body-mass-index; cms: centimeters; ESRD: end-stage renal disease; HAP: human activity profile; MAS: maximum activity score. • Post-HD, the correlation between cBISECF and T2 of TA (r=0.45; p=0.04) and MG (r=0.47; p=0.03) • Post-HD correlation of ADC of LG showed the highest correlation with cBIS ECF (r=0.602; p=0.01) • The paired sample t test indicated significant difference between pre and post HD values of T2 and ADC for TA, MG, LG and soleus Table 2: Association between calf BIS and MRI measures * p<0.05; BIS: bioelectrical impedance spectroscopy; ECF: extracellular fluid; MRI: magnetic resonance imaging. Figure 4: Association between calf BIS ECF and T2 of Tibialis Anterior Figure 5: Association between calf BIS ECF and T2 of Medial Gastrocnemius • We suggest that T2 measures reflect individual skeletal muscle hydration • Calf BIS ECF may not be an appropriate measure to estimate hydration of a single muscle • The pre HD excess plasma volume may have confounded the correlations between cBIS ECF and interstitial ECF measured using MRI acquired T2 for all the muscles investigated prior to the HD treatment • The results support our a priori hypothesis based on fiber type distribution • Tibialis anterior muscle, composed of ~50% type II fibers12 had correlation similar to MG (about ~ 47% type II fibers). The correlation with soleus (least amount of type II fibers13) was smallest • The “ECF outlier” data from a single participant was in accordance to his clinical presentation and hence was included in data analysis We suggest that transverse relaxation times provide best estimates of individual skeletal muscle hydration before and after HD treatment in this population • Jamal SA, Leiter RE, Jassal V, et.al. Impaired muscle strength is associated with fractures in hemodialysis patients. Osteoporos Int. 2006; 17:1390-7. • Johansen KL. Exercise in the end-stage renal disease population. J Am SocNephrol. 2007; 18:1845-4. • Sawant A, House AA, Overend TJ. “Anabolic effect of exercise training in people with end-stage renal disease on haemodialysis: Meta analysis and systematic review.” In submission. • Cleary MA, Sitler MR, Kendrick ZV. Dehydration and symptoms of delayed-onset muscle soreness in normothermic men. J Athl Train. 2006; 40: 36-45. • Kemoun G, Thournie D, Boisson D, Guieu JD. Ankle dorsiflexor delay can predict falls in the elderly. J Rehabil med. 2002; 34:278-83. • Zhu F, Sarkar S, Kaitwatchrachai C, et. al. Methods and reproducibility of measurement of resistivity in the calf using regional bioimpedance analysis. Blood Purif. 2003; 21:131-6. • Zhu F, Kuhlmann MK, Sarkar C, et.al. Adjustment of dry weight in hemodialysis patients using intradialytic continuous multifrequencybioimpedance of the calf. Int J Artif Organs. 2004; 27:104-9. • Holl N, Echaniz-Laguna A, Bierry G et al. Diffussion weighted MRI of denervated muscle: A clinical and experimental study. Skeletal Radio. 2008; 37:1111-7. • Yanagisawa O, Shimao D, Maruyama K, et. al. Diffusion-weighted magnetic resonance imaging of human skeletal muscles: gender-, age-, and muscle-related differences in apparent diffusion coefficient. MagnReson Imaging.2009;27:69-78. • Fix A, Daughton D. Human Activity Profile. Odessa, FL: PsychologicalAssessmentResources Inc.; 1988. • Hall WH, Ramachandran R, Narayan S, et. al. An electronic application for rapidly calculating Charlson comorbidity score. BMC Cancer. 2004; doi:10.1186/1471-2407-4-94 • PortneyGL, Watkins MP. Foundations of clinical research: Applications to clinical practise. 2nd Edition, Prentice Hall, 1999. • Henriksson-Larsen K, Friden J, Wretling M-L. Distribution of fibre sizes in human skeletal muscle. An enzyme histochemical study in m tibialis anterior. ActaPhysiol Scand. 1985; 123:171-7. • GollnikPD, Sjodin B, Karlsson J, et. al. Human soleus muscle: a comparison of fiber composition and enzyme activities, with other leg muscles. Pfliigers Arch. 1974; 348:247—55. • Albrachta K, Arampatzisa A, Baltzopoulosb V. Assessment of muscle volume and physiological cross-sectional area of the human triceps surae muscle in vivo. J Biomech. 2008; 41:2211-8 • Ikizler TA, Himmelfarb J. Muscle wasting in kidney disease: let’s get physical. J Am SocNephrol. 2006; 17:2097-8. • Di Iorio B, Cillo N, Gaspare De Santa N. Charlsoncomorbidity index is a predictor of outcomes in incident hemodialysis patients and correlates with phase angle and hospitalization. Int J artif Organs. 2004; 27:330-6. • Renal Research Institute New York, for providing training, equipment and software for measurement of calf BIS measures. • The Kidney Foundation of Canada for providing funding for this study. • Anuradha Sawant is recipient of The KFOC Allied Health Doctoral Fellowship. • Our participants for their time and enthusiasm to take part in this study. Conclusion Purpose References Methods A priori Hypothesis Acknowledgements Results


















