Download
1 / 78
1k likes | 1.7k Vues
Lecture 2 and 3 Leukopoiesis, bone marrow, WBC disorders Abdulkarim Aldosari. O bjectives. Define and describe Leukopoiesis List proper cell maturation of the myeloid and lymphoid series Characterize changes in neutrophil count and morphology that develop in response to infections

E N D
Lecture 2 and 3 Leukopoiesis, bone marrow, WBC disorders AbdulkarimAldosari
Objectives • Define and describe Leukopoiesis • List proper cell maturation of the myeloid and lymphoid series • Characterize changes in neutrophil count and morphology that develop in response to infections • Characterize the sequence of events that occur during phagocytosis • Define neutropenia and identify causes • Describe the etiology and neutrophil morphology of Chediak-Higashi syndrome, May-Hegglin, Alder-Reilly, and Pelger-Huet anomalies. • Describe chronic granulomatous disease • Compare and contrast white cell anomalies in regard to morphology • Define monocytosis and lymphocytosis • List disorders associated with monocytosis and lymphocytosis • Distinguish between absolute and relative, benign and malignant lymphocytosis • Describe infectious mononucleosis
White blood count Normal indices for WBC DifferentialAbsolute counts Lymphocytes 20-44% 1.2-3.4 x 103/µl Monocytes 2-9% 0.11-0.59 x 103/µl Neutrophils 50-70% 1.4-6.5 x 103/µl Bands 2-6% 0-0.7 x 103/µl Eosinophils 0-4% 0-0.5 x 103/µl Basophils 0-2% 0-0.2 x 103/µl Absolute count = %/100 x WBC
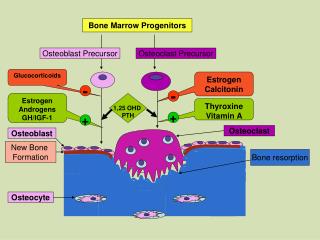
Leukopoiesis • Leukopoiesis-is a form of hematopoiesis • White blood cells (WBC, or leukocytes) are formed in bone marrow • WBCs are formed from the differentiation of pluripotent hematopoietic stem cells which give rise to several cell lines with more limited differentiation potential • Regulated by the production of interleukins and colony-stimulating factors (CSF). Two main groups of WBCs: • Myeloid cells (granulocytes) • Large cells with lobed nuclei and visibly staining granules; all are phagocytic • Neutrophils • Eosinophils • Basophils • Monocytes • Lymphoid cells • Agranulocytes -lack visibly staining granules
Myelopoiesis (granulocytopoiesis) • Hematopoietic system produces enough neutrophils (~1.3 x 1011 cells per 80-kg person per day) to carry out physiologic functions • Also has a large reserve stored in the marrow, which can be mobilized in response to inflammation or infection • An increase in the number of blood neutrophils is called neutrophilia • Presence of immature cells is termed a shift to the left • A decrease in the number of blood neutrophils is called neutropenia • Mature neutrophils, eosinophils, basophils have similar patterns of proliferation, differentiation, division, storage in BM and delivery to PB.
Proliferation Maturation Storage Functional pools
Blood Cells in peripheral blood • Only formed elements that are complete cells • Make up less than 1% of total blood volume
Neutrophils in peripheral blood • Most numerous type of leukocyte = 50-70% • Diameter 10-12µm • 3000-7000 cells/mm3 • Most mobile cell lines in human • Chemically attracted to sites of inflammation • Cytoplasmic granules – containing enzymes • > killing and digestion of bacteria and fungi • Active phagocytes of bacteria
Maturation of neutrophils • 14 days to develop • Mature cells leave the marrow > moving through transiently formed pores in endothelial cells • Become part of functional pool > half circulating cells or half marginated cells (line blood vessel walls) • After few hours > leave blood for tissues and body cavities as directed by chemotactic factors in response to inflammation or infection • Once in tissues they do not re-enter circulation of marrow • As they leave blood, they are replaced by other cells from BM
Maturation of neutrophils The myeloblast is the first recognizable precursor cell • Round nucleus, reddish blue, smooth nuclear membrane, • Fine, delicate, evenly stained chromatin, • Nucleoli – 0-2 • Bluish, non-granular cytoplasm • N:C = 7:1 – 5:1, central • 15 to 20 µm • Not present in normal PB • Normal marrow – 0-2 % • Followed by the promyelocyte
Maturation of neutrophils The promyelocyte evolves when the primary, or azurophil, lysosomal granules are produced • 12-24 µm • Not present in normal PB, 1-4% in BM • N:C = 5:1 to 3:1 • Chromatin – finely granular • Nucleoli – faintly visible or not distinct • Blue cytoplasm, with lighter zone near nucleus • Cytoplasm not indented by adjacent cells • The promyelocyte divides to produce the myelocyte
Maturation of neutrophils • The myelocyte- cell responsible for the synthesis of the specific, or secondary, granules • Nucleus- round, oval, flattened on one side, eccentrically located • Chromatin strand – condensed, partly clumped, thickened, unevenly stained • Nucleoli – absent/rare • Last myeloid precursor capable of division • Smaller than promyelocytes • N:C – 2:1 to 1:1 • 10-18 µm • Cytoplasm more pink • Not seen in normal PB, 5-20% in BM • End of proliferation pool of cells
What are these granules? • The primary granules contain hydrolases, elastase, myeloperoxidase, cathepsin G, cationic proteins and bactericidal/permeability-increasing protein - important for killing gram-negative bacteria • Azurophil granules also contain defensins, a family of cysteine-rich polypeptides with broad antimicrobial activity against bacteria, fungi, and certain enveloped viruses
What are these granules? • Specific, or secondary, granules-contain lactoferrin, vitamin B12–binding protein, membrane components of the reduced nicotinamide-adenine dinucleotide phosphate (NADPH) oxidase required for hydrogen peroxide production, histaminase, and receptors for certain chemo-attractants and adherence-promoting factors (CR3) and other membrane receptors • The secondary granules do not contain acid hydrolases and therefore are not classic lysosomes • Secondary granule contents are released extracellularly, and their mobilization is important in modulating inflammation
Maturation of neutrophils • As maturation proceeds, nucleus becomes more indented (kidney bean shaped) = metamyelocyte • The proliferation phase from myeloblast to the metamyelocyte takes about 1 week • Indentation of nucleus = less than half the width of the round nucleus • Chromatin – clumped • Cells do not divide • Maturation pool of WBCs in BM • Do not have nucleoli • N:C = 1:1, central or eccentric • Small pinkish granules • Smaller than myelocytes = 10-18 µm • Absent in normal PB, 5-20% in BM
Maturation of neutrophils • Band neutrophil formed when the nuclear indentation is greater than the width of the nucleus • From metamyelocyte to mature neutrophil takes another week • Appearance of horseshoe, central or eccentric • May appear twisted or folded • Nuclear chromatin is pyknotic • Ends have a dark condensed mass • N:C = 1:1 to 1:2 • Cells are smaller than metamyelocytes • 10-16 µm • Maturation pool in BM 10-35% • In PB 2-6%
Maturation of neutrophils • Segmented neutrophil – two to five nuclear lobes connected by a thin filament/strand • Nuclear chromatin is purplish-red, clumped • N:C = 1:3 • Cells are smaller than metamyelocytes • 10-16 µm • Maturation pool in BM 5-15% • In PB 50-70%
Maturation of neutrophils • Borderline cells should be classified as the more mature cell • In BM – proliferation pool ( committed stem cell- blast- promyelocyte-myelocyte) • In BM – maturation pool (metamyelocyte and bands) • In BM – storage pool (mature cells for release into peripheral blood)
Neutrophil function The main function of neutrophils – internalization of microorganisms Phagocytosis-three phases: • Migration and diapedesis (outward passage of cells through intact vessel walls) • Opsonization and recognition • Ingestion, killing and digestion (phagocytosis)
Neutrophil function Step 1. Migration Bacteria in tissue > sends out signal via chemoattractants > stimulate changes in neutrophil morphology and migration > neutrophil clings to the endothelial receptors > penetrates through the endothelial cells via diapedesis > neutrophil migrates to site of infection = chemotaxis Three modes of neutrophil migration Locomotion – random, non-directional movement of neutrophils as they roll along vessel endothelium until site of infection or injury Chemokinesis – chemoattractants accelerate the migration speed of neutrophils Chemotaxis – directional migration to site of infection
Neutrophil function Step 2. Opsonization Neutrophils recognize and attach to infecting organism via circulating Igs and activated complement components which coat the surface of the bacteria Neutrophil membranes carries receptors for the Fc fragment of Igs and activated complement only. Ingestion will not take place without the presence of membrane-bound Igs
Neutrophil function Step 3. Phagocytosis: ingestion, killing, digestion Ingestion begins as soon as neutrophil receptor and bacteria bind together > pseudopods envelop microbe > form vacuole = phagosome > cytoplasmic granules fuse to phagosome, release contents > lytic action of enzymes > killing and digestion of microbe = Killing and digestion mechanism: • non- oxygen dependent – lysing of bacterial cell wall by lysosomal and proteolytic enzymes • Oxygen dependent (respiratory burst/oxidative burst)-rapid release of NADPH oxidase > production of reactive oxygen species (superoxide and hydrogen peroxide) from neutrophils and monocytes as they come into contact with different bacteria or fungi.
Disorders of neutrophils • Neutrophils -the first line of defense against most bacterial pathogens. • Requires that the host have sufficient numbers of neutrophils that respond to chemotactic stimuli and ingest and kill bacteria • Classified as quantitative and qualitative • Quantitative • Neutropenia = decease in number < 1.5 x 109/L • Neutrophilia = increase in number > 30,000/mm3or 30 x 109/L • Qualitative • Neutrophil dysfunction – impaired migration or altered bacteriocidal activity
Neutrophilia • Absolute count > 30,000/mm3 or 30 x 109/L • A classic response to infections and inflammation • Accelerated release of neutrophils from BM • Accompanied by a “left shift” = increase in the number of immature cells (metamyelocytes and bands) in the PB • To be differentiated from an ↑ in circulating neutrophils and immature cells due to chronic myeloid leukemia CML and other myeloproliferative disorders
Differentiate neutrophilia • Major distinction = immature cells limited to metamyelocytes and bands in infections but more immature cells (myelocytes, promyelocytes and blasts) present in neoplastic processes. • LAP – leukocyte alkaline phosphatase is ↑ in leukemoid reactions, i.e. reactions due to an infection, ↓ in CML. Done by cytochemical staining. A leukemoid reaction is an increase in white blood cell count similar to what occurs in people with leukemia. However, the reaction is actually due to an infection or another disease and is not a sign of cancer. Blood counts will usually return to normal when the underlying condition is treated. • Other cause of neutrophilia – tissue necrosis, metabolic disorders, stress, rigorous exercise, pregnancy, smoking, trauma, hemolysis, postsplenectomy • Various reactive changes that occur to the neutrophil during infection also occur during these others causes
Neutrophilic morphology Changes in the morphology of neutrophils that occur during a leukemoid reaction Toxic granulation • Associated with sever infections • Granules enlarge and take on darker staining properties • Usually peroxidase-positive primary granules Dohle bodies • Usually accompanies toxic granulation • Pale blue inclusions at periphery of cytoplasm • Aggregated strands or rough endoplasmic reticulum Vacuolated cytoplasm Ingested microorganisms
Neutropenia Absolute decrease in the number of circulating neutrophils < 1.5 x 109/L Mild – 1.0-1.5 x 109/L Moderate – 0.5-1.0 x 109/L Severe - < 0.5 x 109/L Life threatening - <0.2 x 109/L Not normally the only indicator of disease > should be correlated with pt history and other clinical findings and lab results. Due to recurrent bacterial infection – Staph Aureus, Strep viridans, Gram negative enteric bacteria Occur in the cutaneous and soft tissues > spread to the blood stream
Neutropenia Due to increased destruction or removal of neutrophils – in PB Infections, immune disorders Maturation defect – impaired BM release Megaloblastic anemia Proliferation defect – decreased production Aplastic anemia BM replacement disorders Drugs reactions Myeloablative therapy – radiation therapy BM fibrosis Abnormal distribution Hypersplenism Can be acquired or congenital
Acquired neutropenia Infections • mostly viral – influenza A ,B, rubella, herpes simplex, hepatitis A, B, and RSV • neutropenia appears during first few days of infection – within 24 to 48 hrs Immune mediated • Anti-neutrophil antibodies - alloantibodies or autoantibodies • Similar to RBC hemolytic disease of the newborn • Antigens shared by fetus and father, absent from mother, mother develops ab which cross placenta > destroys fetal neutrophils • Autoantibodies- rheumatoid arthritis, systemic lupus, chronic hepatitis Treatment – antibiotics for infections, prednisone for autoimmune response
Congenital neutropenia Defects in genes encoding ribosomal proteins (SBDS, RMRP) and mitochondrial proteins (AK2, TAZ) are associated with congenital neutropenia syndromes Some variants of congenital neutropenia may be due to mutations in genes controlling glucose metabolism (SLC37A4, G6PC3) or lysosomal function (LYST, RAB27A, ROBLD3/p14, AP3B1, VPS13B). Patients with congenital neutropenia are prone to severe and recurrent bacterial infections such as otitis media, bronchitis, pneumonia, osteomyelitis, or cellulitis. Long-term neutropenic states also predispose to fungal infections. http://asheducationbook.hematologylibrary.org/content/2009/1/344.full
Qualitative disorders of neutrophils Hereditary abnormalities in function > bacterial infections Familial due to a general metabolic defect Pathophysiology is unknown Functional defects are classified by the general type of defect • Phagocytic/killing defects • Motility/chemotaxis defects • Granule function and structure defect • Adhesion defects
Qualitative disorders of neutrophils Classes of qualitative neutrophil disorders • Cytoplasmic granules • Disturbances of the respiratory burst • Chemotaxis WBC counts are variable PB smear is not used to differentiate the disorders except for the large granules present in Chediak-Higashi Syndrome
Chediak-Higashi Syndrome • Rare autosomal recessive disease -one in which neutrophils, monocytes, and lymphocytes contained giant cytoplasmic granules • Dysfunction characterized by increased fusion of cytoplasmic granules • The presence of giant granules in the neutrophil interferes with their ability to traverse narrow passages between endothelial cells.
Chediak-Higashi Syndrome • The decrease in phagocytosis results in recurrent pyogenic infections, partial albinism and peripheral neuropathy • Patients have light skin and silvery hair, solar sensitivity and photophobia – albinism • Other features of the disease include neutropenia, thrombocytopenia, natural killer cell abnormalities • Patients with this syndrome exhibit an increased susceptibility to infection due to defects in neutrophil chemotaxis, degranulation, and bactericidal activity.
Clinical Features of CHS • The infections involve the mucous membranes, skin, and respiratory tract. • Susceptibility to both gram-positive and gram-negative bacteria as well as fungi, with Staphylococcus aureus being the most common infecting organism. • The neuropathy may be sensory or motor in type, and ataxia may be a prominent feature. • Covers two of the four disorders – granule structure/function and chemotaxis defect • Treatment – antimicrobial therapy, ascorbic acid
Chronic granulomatous disease Best understood disease of neutrophil function • Mutation in NADPH oxidase > ineffective bacterial killing • Mostly X-linked recessive – affects mostly boys by first year • Failure in the activation of the respiratory burst > little or no superoxide production • Mutation in the gene encoding the NADPH oxidase
Chronic granulomatous disease • Clinical picture – recurrent pulmonary infections, infected eczematous rash, neutrophilia instead of neutropenia • Diagnosis – nitroblue tetrazolium test NBT • It is negative in CGD= does not turn blue. The higher the blue score, the better the cell is at producing reactive oxygen species • Depends upon the direct reduction of NBT to the insoluble blue compound formazan by NADPH oxidase; NADPH is oxidized in the same reaction • Treatment – prophylactic antibiotic therapy, gamma interferon, BM and stem cell transfusions
Abnormal neutrophil morphology Acquired Hypersegmentation – five or more nuclear lobes • Megaloblastic anemia • Myeloid malignancies (AML, Myelodysplastic syndromes) Pseudo-Pelger-Huet anomaly - Hyposegmentation 70-90% Bilobed or no lobulation Secondary to • Myeloid malignancy • Drugs –sulfonamides etc. Nuclear chromatin very coarse and condensed Dumbbell shaped Versus true Pelger-Huet – autosomal dominant, inherited disorder
Abnormal neutrophil morphology Inherited • Alder-Reilly anomaly • Prominent, dark staining coarse cytoplasmic granules, • Similar to toxic granulation but larger • May-Hegglin anomaly • Dark blue staining cytoplasmic inclusions in neutrophils • Larger than Dohle bodies; thrombocytopenia, giant platelets • Chediak-Higashi syndrome • Giant granules in granulocytes • Pelger-Huet anomaly – • Bilobed or non-segmented nuclei
Eosinophils • Large, round, secondary, refractile granules staining orange to reddish-brown > takes on the acid eosin stain • Relatively uncommon – 0-3% in BM, 0-4% in PB • Granules contain hydrolytic enzymes – peroxidase, acid phosphatase, aryl sulfatase, beta-glucuronidase, phospholipase, cathepsin, ribonuclease
Eosinophils • Diurnal variation in circulating eosinophils- % ↑ at night and ↓ in the morning • Bilobed nucleus • 10-14µm • Lasts 5 days in circulation • Stem cell kinetics not as well known as for neutrophils
Eosinophils • Substances in the granules of Eosinophils become cytotoxic when they are released on the surface of parasites. • Eosinophils are not phagocytic, but they intoxicate nematodes and other parasites and bacteria. • The cytotoxic substances are major basic protein, which kill helminthes, eosinophil cationic protein (an extremely efficient killer of parasites and potent neurotoxins) and eosinophil peroxidase (kills bacteria, helminthes and tumor cells). • Eosinophils are involved in hypersensitivity reactions.
Basophils • Maturation, division and proliferation similar to neutrophils • Nucleus is masked by large basophilic granules • Granules = histamine and heparin, are water soluble • Respond to acute and delayed allergic reactions • Granules formed in the myelocytic stage and continue to be produced throughout later stages of maturation
Basophils • Mature basophils rarely have more than two segments • Circulate for few hours then migrate into skin, mucosa and other serous membranes • All stages are smaller than neutrophils • In BM 0-1%, In PB 0-2% • Diurnal variation in circulating basophils- % ↑ at night and ↓ in the morning • Mast cells = tissue basophils
Basophils • Circulating basophils and mast cells residing in the tissues are morphologically similar • Granules contain histamine and other vasoactive amines. • Cells are involved in hypersensitivity reactions. • The binding of IgE to the cells stimulate the release of histamine, but also of prostaglandins, leucotrienes and cytokines. • Some mast cell contains trypsin and cytoplasmic IgE and others contains both trypsin and chymotrypsin.
Eosinophilia and Basophilia Eosinophilia • Mostly caused by – allergic reactions in developed countries • Parasitic infection – helminthic • Also in malignant hematopoietic disorders, skin disorders, pulmonary disorders, inflammatory disorders • Disappears with the resolution of the disease Basophilia • Secondary to allergic reactions • Malignant hematological disorders - CML