Download
1 / 32
330 likes | 474 Vues
Deep Brain Stimulation(DBS). Professor: Dr.Towhidkhah Presented by: Kayvan Mojtahedi. Introduction. Components & Placement. Surgery. Advantages of Deep Brain Stimulation. Possible Disadvantages. Potential Complications & Side Effects. Anatomical Targeting. PD. PD:DBS.

E N D
Deep Brain Stimulation(DBS) Professor:Dr.TowhidkhahPresented by: KayvanMojtahedi
Introduction Components & Placement Surgery Advantages of Deep Brain Stimulation Possible Disadvantages Potential Complications & Side Effects Anatomical Targeting PD PD:DBS Effects of low-frequency stimulation of the subthalamic nucleus on movement in Parkinson's disease
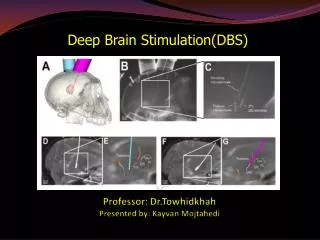
Deep Brain Stimulation In neurotechnologydeep brain stimulation (DBS) is a surgical treatment involving the implantation of a medical device called a brain pacemaker, which sends electrical impulses to specific parts of the brain. The Food and Drug Administration (FDA) approved DBS as a treatment for essential tremor in 1997, for Parkinson's disease in 2002, and dystonia in 2003. DBS is also routinely used to treat chronic pain and has been used to treat various affective disorders, including major depression. A) DBS systems are permanently implanted with a pulse generator in the chest and a four contact electrode stereotactically placed in the brain. Post-operative MR is used to identify STN and local structures, as well as electrode location.
Deep Brain Stimulation Components & Placement i. The implanted pulse generator (IPG) ii. The lead iii. The extension Electrodes are placed in the thalamus (for essential tremor and multiple sclerosis) or in the globuspallidus (for Parkinson's disease). DBS leads are placed in the brain according to the type of symptoms to be addressed. For non-Parkinsonianessential tremor the lead is placed in the ventrointermedial nucleus (VIM) of the thalamus. For dystonia and symptoms associated with Parkinson's disease (rigidity, bradykinesia/akinesia and tremor), the lead may be placed in either the globuspallidus or subthalamic nucleus.
Deep Brain Stimulation The IPG is a battery-powered neurostimulator encased in a titanium housing, which sends electrical pulses to the brain to interfere with neuralactivity at the target site. The lead is a coiled wire insulated in polyurethane with four platinumiridium electrodes and is placed in one of three areas of the brain. The lead is connected to the IPG by the extension, an insulated wire that runs from the head, down the side of the neck, behind the ear to the IPG, which is placed subcutaneously below the clavicle or in some cases, the abdomen.[ Pacemaker device (called an impulse generator, or IPG) implanted under the skin of the chest, below the collarbone.
Deep Brain Stimulation (Surgery) All three components are surgically implanted inside the body: Under local anesthesia, a hole about 14 mm in diameter is drilled in the skull and the electrode is inserted, with feedback from the patient for optimal placement. (The right side of the brain is stimulated to address symptoms on the left side of the body and vice versa.) The installation of the IPG and lead occurs under general anesthesia. Insertion of electrode during surgery
a: Variation of the lead position in the xz-plane: Position A is along the symmetry axis of the scanner, position C is along the RF coils, and position B is in between. In each case the lead is parallel to the z-axis. b: Variation of the lead position in the xy-plane: after the lead exits the phantom, it is fixed at the tunnel wall of the scanner under different angles. From there it is led outside the scanner parallel to its z-axis.
Photographs illustrating the consecutive steps in the described DBS-electrode anchoring technique for patients. After satisfactory DBS-electrode placement the dura is sealed with a drop of fibrin glue (A and B). A 20mm long piece of a ventricular catheter cut slit open is fitted around the electrode (C). The burr hole is filled with BioGlue® fixating the electrode to the burr hole, and the applied electrode cover to the electrode and the burr hole (D). The electrode stiletto is removed and the electrode released from the stereotaxic device (E). The covered electrode is fixated to the calvarium with a 3×4 hole Lorentz titanium microplate placed over the burr hole and screwed onto the skull by four 4mm titanium screws (F).
a: Experimental setup. The lead connects the pulse generator outside the scanner room and the electrode inside the phantom. The phantom is positioned at the isocenter of the scanner. Induced voltage is measured at the connecting lead outside the scanner room. Measurement points for the temperature are equally spaced along the electrode and the lead. b: Percutaneous placement of the lead before the final implantable pulse generator (IPG) is implanted into the patient’s chest. The lead penetrates the scalp and is coupled to the test stimulator by the connector.
What Are the Advantages of Deep Brain Stimulation? It does not require purposeful destruction of any part of the brain and therefore, has fewer complications than thalamotomy and pallidotomy. The electrical stimulation is adjustable and can be changed as the person's disease changes or his or her response to medications change. No further surgery is necessary to make the adjustments. Another significant advantage of deep brain stimulation relates to future treatments. Destructive surgery, such as thalamotomy or pallidotomy, may reduce the persons potential to benefit from future therapies. For example, future brain cell transplantation may be of great help to people with Parkinson's disease. There is concern that a pallidotomy or thalamotomy may prevent patients from benefiting from brain cell transplantation. This would not be the case with deep brain stimulation, as the stimulator could be turned off. Deep brain stimulation is a relatively safe procedure. The procedure can treat all the major symptoms of Parkinsons disease. Daily living tasks and quality of life are also improved. With subthalamic nucleus stimulation, medications can usually be reduced. The stimulator can also be turned off at any time if deep brain stimulation is causing excessive side effects.
Possible Disadvantages • Potential complications and side effects: Increased risk of infection. The implantation of any foreign object carries that risk. • Additional surgery may be needed if the equipment stops working or for battery replacement • Additional time on the part of the patient and health care provider to program device and adjust medications • Device may interfere with antitheft devices, refrigerator door magnets.
Potential Complications & Side Effects a. The possibility of apathy, hallucinations, compulsive gambling, hypersexuality, cognitive dysfunction, and depression. However, these may be temporary and related to correct placement and calibration of the stimulator and so are potentially reversible. (There is a 2%-3% risk of a serious and permanent complication such as paralysis, changes in thinking, memory and personality, seizures, and infection.) b. Because the brain can shift slightly during surgery, there is the possibility that the electrodes can become displaced or dislodged. This may cause more profound complications such as personality changes, but electrode misplacement is relatively easy to identify using CT or MRI. There may also be complications of surgery, such as bleeding within the brain.
Anatomical Targeting Pallidum and putamen are shown. Stimulation has varying effects on different symptoms in internal globuspallidus(GPi) and external globuspallidus(GPe) (Bejjani et al., 1997; Krack et al., 1998; Yelnik et al., 2000).
Fig. 3. (a) Model of the DBS lead with four contacts centered in the STN, surrounded by white fiber tracts (zonaincerta (ZI), Fields of Forel (FF), and internal capsule (IC)) and grey matter. Distribution of (1) electric potential (V); (2) electric field (ΔV); and (3) the activating function (ΔV^2) generated in the subthalamic nucleus and the surrounding fiber tracts during (b) monopolar stimulation (V=-1) applied through Contact 1, (c) bipolar stimulation (Contact 1 at V=-0.5; Contact 2 at V=0.5); (d) bipolar stimulation (Contact 1 at V =0.5 V, Contact 2 at V=-0.5 V), and (e) tripolar stimulation (Contacts 0 and 2 at V =0.05, Contact 1 at V=-0.5). ΔV and ΔV^2 have both positive and negative components, but the magnitudes are shown here. Positive ΔV^2 results in depolarization and negative ΔV^2 results in hyperpolarization of the surrounding neural elements. CNS gray matter has a conductivity of 0.2 S/m (Li et al., 1968; Ranck, 1963). CNS white matter has conductivities of 1 S/m in the direction parallel to the fibers and 0.1 S/m in the direction perpendicular to the fibers (Nicholson, 1965).
PD Kinds of Treatments(4.1,P.P of YasharSarbaz): Parkinson’s Disease 1-1. Medical treatment 1-2. Deep Brain Stimulation
PD PD & it’s symptoms Reason of PD: Loss of nerve cells in substantia nigra pars compacta Low level of Dopamine in patient’s brain Changing activity of other blocks
PD PD and it’s symptoms Symptoms of PD: • Hypokinesia Akinesia: lack of slowness of spontaneous and associative movement Rigidity: increased tone on passive manipulation of joints • Tremor:rhythmic,involuntary,oscillatory movement around 4-6 Hz
PD PD:DBS Target of Stimulation: • GPi: The GlobusPallidus Internal • STN:TheSubthalamic Nucleus • Vim: The Ventro-Intermediate nucleus Thalamus
Fig. 3. (a) Model of the DBS lead with four contacts centered in the STN, surrounded by white fiber tracts (zonaincerta (ZI), Fields of Forel (FF), and internal capsule (IC)) and grey matter. Distribution of (1) electric potential ðVÞ; (2) electric field ðDVÞ; and (3) the activating function ðD2VÞ generated in the subthalamic nucleus and the surrounding fiber tracts during (b) monopolar stimulation ðV ¼ 21Þ applied through Contact 1, (c) bipolar stimulation (Contact 1 at V ¼ 20:5; Contact 2 at V ¼ 0:5Þ; (d) bipolar stimulation (Contact 1 at V ¼ 0.5 V, Contact 2 at V ¼ 20.5 V), and (e) tripolar stimulation (Contacts 0 and 2 at V ¼ 0.05, Contact 1 at V ¼ 20:5Þ: DV and D2V have both positive and negative components, but the magnitudes are shown here. Positive D2V results in depolarization and negative D2V results in hyperpolarization of the surrounding neural elements. CNS gray matter has a conductivity of 0.2 S/m (Li et al., 1968; Ranck, 1963). CNS white matter has conductivities of 1 S/m in the direction parallel to the fibers and 0.1 S/m in the direction perpendicular to the fibers (Nicholson, 1965). PD Characteristics of the common DBS signal: • Frequency greater than 100 • Pulse width about 90 • Amplitude of stimulation voltage nearly 3 v
PD Effects of low-frequency stimulation of the subthalamic nucleus on movement in Parkinson's disease Abstract Introduction Materials and methods: Patients and surgery: 1. The DBS electrode used was model 3389 (Medtronic Neurological division, Minneapolis, USA) with four platinum–iridium cylindrical surfaces (1.27 mm diameter and 1.5 mm length) and a centre-to-centre separation of 2 mm. Contact 0 was the most caudal and contact 3 was the most rostral. The intended coordinates at the tip of contact 0 were 10–12 mm from the midline, 0–2mm behind the midcommissural point and 3–5mm below the anterior commissural–posterior commissural line. 2. Correct placement of the DBS electrodes in the region of the STN was further supported by: [1] effective intra-operative macrostimulation; [2]post-operative T2-weighted MRI compatible with the placement of at least one electrode contact in the STN region; [3] significant improvement in UPDRS motor score during chronic DBS off medication (22.7±3.0) compared to UPDRS off medication with stimulator switched off (52.6±4.8; p‹0.00001, paired t-test).
PD Protocol: 3. All patients were assessed after overnight withdrawal of antiparkinsonian medication. They were studied when the stimulator was switched off and during bilateral STN stimulation at 5 Hz, 10 Hz and 20 Hz. Task 4. Tapping was performed in two runs of 30 s, separated by ∼30-s rest and each hand tested separately (giving four runs per condition). The number of taps made with the index finger in 30 s was recorded. Statistics 5. The results of the tapping task in patients were analyzed according to their baseline performance (e.g. without stimulation). The lower limit of normal baseline performance was obtained by testing ten healthy age matched control subjects (20 sides, 4 males, mean age 57 years, range 52–64 years) using the same tapping task. The mean tapping rate in this control group was 162 taps/30 s. 6. The lower limit of the normal range (e.g. mean−[2×standard deviation]) in this control group was 127 taps per 30 s. The 35 tapping sides studied in the 18 patients were accordingly divided into those with baseline performance within normal limits (n=17; the mean tapping performance across this group, 157 taps/30 s, was still lower than the mean tapping performance in healthy subjects) and those with baseline tapping rates lower than normal limits (n=18; mean tapping performance 58 taps/30 s). 7. Greenhouse–Geisser corrections: Means±standard error of the means(SEM)
PD iv. Result Fig. 1. Effects of stimulation frequency on tapping rate off medication. Mean (±SEM) tapping rate off (‘0 Hz’) and on stimulation at 5, 10 and 20 Hz on those sides (n=17) with baseline tapping performance within normal range (tapping off DBS›127 taps in 30 s) (A) and below normal range (n=18) (B). In those patients with baseline performance within normal limits, tapping rate was significantly slower during stimulation at 5 and 20 Hz than without stimulation and there was a similar trend for the 10-Hz stimulation. On those sides with baseline performance below normal limits no significant differences between the different stimulation frequencies were found.
PD Fig. 2. Effects of stimulation frequency on variability of tapping rate off medication. Mean (±SEM) coefficient of variation (CV) of the intervals between taps off (‘0 Hz’) and on stimulation at 5, 10 and 20 Hz in patients with baseline tapping performance within normal range. CV of tap intervals during stimulation at 5 and 10 Hz significantly increased compared to no stimulation.
PD V. Discussion 8. We have shown that STN DBS at a variety of low frequencies can slow distal upper limb movements in PD patients with relatively preserved baseline tapping function at the time of study. The effect was present with DBS at 5 Hz and 20 Hz in line with previous studies (Chen et al., 2007; Fogelson et al., 2005; Moro et al., 2002), and there was a trend towards a similar effect with stimulation at 10 Hz (Timmermann et al., 2004). 9. The susceptibility of basal ganglia–cortical loops to the effects of excessive synchronization may be elevated across a broad low-frequency band in parkinsonian patients. 10. Only DBS at 5 and 10 Hz increased temporal variability, whereas DBS at 20 Hz selectively decreased tapping rates without changing tapping variability. VI. Acknowledgments 11. This work was supported by research grants from the Medical Research Council (UK),Wellcome Trust (UK), Fondation pour la RechercheMedicale (France), Chang GungMemorial University Hospital (Taipei, Taiwan) and Parkinson Appeal (UK).
Reference Effects of low-frequency stimulation of the subthalamic nucleus on movement in Parkinson's disease AlexandreEusebio a,1, Chiung Chu Chen a,b,1, Chin Song Lu b, Shih Tseng Lee c, Chon Haw Tsai d, Patricia Limousin a,e, Marwan Hariz a,e, Peter Brown a, a Sobell Department of Motor Neuroscience and Movement Disorders, Institute of Neurology, 8-11 Queen Square, WC1N 3BG London, UK b Department of Neurology, Chang Gung Memorial Hospital and University, Taipei, Taiwan c Department of Neurosurgery, Chang Gung Memorial Hospital and University, Taipei, Taiwan d Department of Neurology, China Medical University Hospital, Taichung, Taiwan e Unit of Functional Neurosurgery, Institute of Neurology, London, UK Received 13 July 2007; revised 29 August 2007; accepted 5 September 2007 Available online 18 September 2007 ii. Deep Brain Stimulation on MedicineNet_com.mht iii. Deep brain stimulation - Wikipedia, the free encyclopedia.mht iv. Powerpoint of YasharSarbaz v. Other CNF & Papers & Journals
PD 1-1.Origion of PD (BG)
The basal nucleii (ganglia) have an inhibitory role in motor control
The basal nucleii (ganglia) have an inhibitory role in motor control
![EVM System Surveillance Presented By: [NAMES] Presented to: [GROUP]](https://cdn2.slideserve.com/3705648/slide1-dt.jpg)