Download
1 / 44
490 likes | 914 Vues
Overview of Disruptive Behavior Problems. Students with disruptive behavior disorders are a heterogeneous group Most are boys However, conduct problems are not uncommon among adolescent girls. Overview of Disruptive Behavior Problems.

E N D
Overview of Disruptive Behavior Problems Students with disruptive behavior disorders are a heterogeneous group Most are boys However, conduct problems are not uncommon among adolescent girls
Overview of Disruptive Behavior Problems • Many youngsters exhibit individual traits and behaviors in early childhood that foreshadow a developmental path leading to more destructive and aggressive behaviors as adolescents and adults
Overview of Disruptive Behavior Problems • One of the difficulties in identifying these disorders is that a certain amount of rowdy play • Risk factors may contribute to the development of these disorders
Overview of Disruptive Behavior Problems • Collectively, these risk factors are producing children and youth who: • A-see violence as a viable means of solving problems • B-don’t respect the rights of others • C-are not socially responsible • d-have not been taught basic manners and social conventions
Overview of Disruptive Behavior Problems • E-don’t value human life as they should RISK FACTORS AND PREDICTORS OF DISRUPTIVE BEHAVIOR DISORDERS • Individual factors that predispose a child to disruptive behaviors include:
Overview of Disruptive Behavior Problems • 1- a difficult temperament • 2-cognitive or learning impairments • 3-neuropsychological problems • 4-mental illness
Overview of Disruptive Behavior Problems Family predictors of disruptive behavior include: • 1-harsh and ineffective parenting • 2-parental antisocial and pathological components • 3-parents with alcohol and drug dependencies • 4-interrupted parenting
Overview of Disruptive Behavior Problems • History of abuse or neglect • Later adoption age • Prenatal drug exposure • Multiple foster placements prior to adoption
Overview of Disruptive Behavior Problems School Factors that may contribute to behavior disorders: 1-academic factors 2-negative relationships with peers and adults 3-punitive school environment
Overview of Disruptive Behavior Problems Community factors include : 1-access to drugs and alcohol 2-exposure to violence 3-lack of educational and employment opportunity 4-acceptance of aggression as a problem solving strategy
Overview of Disruptive Behavior Problems • Treatment Options 1-Results of treatment interventions in residential settings have not transferred to natural setting including the home or school 2-School based group intervention studies have been few in number and the results have shown students with disruptive behavior patterns to be very resistant to treatment
Types of Disruptive Behavior Problems • DSM-IV-TR (Diagnostic and Statistical Manual of the American Psychiatric Association) lists four clinical diagnoses that may be appropriate for students with specific patterns of disruptive behaviors. These include:
Types of Disruptive Behavior Problems • A-Oppositional defiant disorder (ODD) • B-Conduct disorder (CD) • C-Disruptive behavior disorder-not otherwise specified (DBD-NOS) • D-Intermittent explosive disorder (IED)
Oppositional Defiant Disorder (ODD) • DSM describes oppositional defiant disorder as a recurrent pattern of negativistic, defiant, disobedient, and hostile behavior toward authority figures that persist for at least 6 months.
Oppositional Defiant Disorder (ODD) Behaviors of ODD include: 1-losing temper 2-arguing with adults 3-defiance/noncompliance with adult requests 4-deliberately annoying others, blaming others or being easily annoyed 5-angry/resenstful attitude 6-spiteful/vindicyive attitude
Oppositional Defiant Disorder (ODD) • Actively defy rules • Deny responsibility for their behavior • Exploit others for their own gain • Students with ODD seem to thrive on conflict, anger, and negativity from others and are often most difficult with the people they know well
Oppositional Defiant Disorder (ODD) • Prevalence: between 1% and 6% of the population-Surgeon General’s Report • DSM reports it as between 2 and 16% • More common in males who were tempermental or hperactive preschoolers • ODD prevalence after puberty is equal between boys and girls • Generally observed before the age of 8 but may emerge through late adolescence
Oppositional Defiant Disorder (ODD) • Co morbid condition: a condition or disorder occurring concurrently with another disorder • ODD often occurs with ADHD which complicates the diagnosis
Oppositional Defiant Disorder (ODD) • Experts have described ODD as a developmental antecedent to Conduct Disorder (CD) for a significant number of children. • If this occurs the diagnosis should be CD rather than ODD
Conduct Disorder (CD) • DSM describes CD as a repetitive and persistent pattern of behavior in which the basic rights of others or age-appropriate societal norms or rules are violated
Conduct Disorder (CD) • They describe these behaviors as fitting into four groups: • 1-Aggression toward people and animals\2-Harm to property • 3-Deceitfulness or theft • 4-Serious rule violations
Conduct Disorder (CD) Associated features and mental disorders that may occur with CD, as follows: • 1-little empathy or concern for the rights and feelings of others • 2-Frequent misperceptions of others’ intentions as hostile or threatening and responding with aggression
Conduct Disorder (CD) • 3-Callous, lack of feelings of guilt or remorse • 4-Low or overly inflated self esteem • 5-Early onset of risk-taking behavior including sex, drinking, smoking, using drugs
Conduct Disorder (CD) • 6-High rates of suicidal ideation • 7-Lower than average cognitive ability, especially verbal IQ
Conduct Disorder (CD) • The long term prognosis for students with CD is grim • Prevalence between 1 and 4% • More than ¼ to ½ of all individuals with CD go on to become antisocial adults • DSM indicates between 1-10% of the population • Higher than males than females
Conduct Disorder (CD) • CD may be evident as early as preschool, but most significant symptoms emerge from middle childhood through middle adolescence • Childhood-onset CD is most common in males and is frequently preceded by a diagnosis of ODD. Early diagnosis has a poor prognosis • Co morbid conditions with CD
Disruptive aBehavior Disorders-Not Otherwise Specified (NOS) • DBD-NOS is used by DSM to classify children whose behavior is oppositional/defiant or conduct disordered, but does not meet all the required criteria for either ODD or CD.
Intermittent Explosive Disorder (IED) • While the DSM-IV TR does not classify intermittent explosive disorder (IED) as a disorder often diagnosed in childhood or adolescence, it is a diagnosis some students bring with them to school. It is characterized by infrequent, unexpected outbursts of disruptive behavior that result in significant harm to people and/or property.
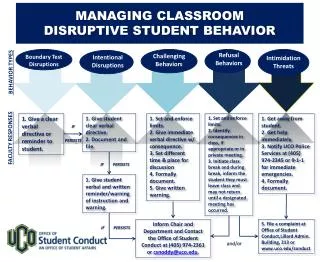
General Rules for Classroom Management • The most important element in classroom management is to have a plan. Answer the following questions to see if you are 'ready for anything'. • 1. What do students do when they come into your classroom in the morning? After recess and lunch?2. What is the consequence for not completing assigned work both in class and out?3. What is the consequence for student(s) interrupting the class or a small group?
General Rules for Classroom Management • 4. How do your students request to leave the room for a drink or to visit the washroom?5. What is the process for the whole class leaving for lunch or recess or to go to the gym?6. What is the consequence for the child who forgets things?
General Rules for Classroom Management • 7. After giving a set of instructions or directions, what is in place for the student(s) that still don't understand?8. How do you respond to the child that keeps leaving his/her seat?9. How will your students know about acceptable voices/noise levels to use for the various activities?
General Rules for Classroom Management • Basic psychology of children with behavior disorders-What the teacher needs to know. • Level I Behavior Disorders • Level II Behavior Disorders
Management of Conduct Disorders • The youth at highest risk of extreme violence may be the conduct disordered child. • Remember that the hallmark of being a conduct disorder (c.d.), is having no heart, no conscience, no remorse.
Management of Conduct Disorders • Only a mental health professional can diagnose a conduct disorder for sure, but being aware that you may have a conduct disordered child in your class or group, is important to ensuring your safety, along with the safety of your kids, because you work with conduct disorders completely differently than other kids.
Management of Conduct Disorders • Since the c.d. child has little relationship capacity, you should not use relationship-based approaches with a diagnosed conduct disorder.
Management of Conduct Disorders • It would be insensitive to call a conduct disorder a "baby sociopath," but that is close to what the term means. It means that the child acts in ways that appear to be seriously anti-social, and the concern is that the child may grow up to be a sociopathic type of person
Management of Conduct Disorders • Since this child cares only about himself (c.d.'s are predominately male), there are little brakes on this child from serious or extreme violence.
Management of Conduct Disorders • DO'S: • *The main point we give in our classes is that these children operate on a cost-benefit system, and that to control your c.d. kids, you must keep the costs high, and benefits low.
Management of Conduct Disorders • *Your goal is to teach them that when they hurt others, it often hurts them too. All interventions must be in the context of "I-Me," because that is all this kid is capable of caring about.
Management of Conduct Disorders • Don't: have a heart-to-heart relationship. • *Don't work on building trust. • *Don't put an emphasis on compassion, caring, empathy, values, morals. • *Don't expect compassionate behavior. • *Don't trust. • *Don't give second chances. • *Don't believe they care or feel remorse.
Management of Conduct Disorders • Conduct disorders are "wired" differently than other students. That means that they may not be able to care. Because of that difference, the following interventions will fail: character ed, values clarification, empathy building, second chances, making amends, and more-- far too many to list here. These methods fail because the child must care about others if these techniques are to work.
Management of Conduct Disorders • These approaches are absolutely fine for other types of children, but will never be of value with C.D.s. In fact, these methods make the situation worse because they communicate to these children that you don't understand who they are, and don't understand how to control them. That perception generally leads these youngsters to believe that they may be able to do whatever they want without having to deal with consequences that would be of significant concern to them.