Download
1 / 66
670 likes | 698 Vues
Explore the essential functions and processes of the urinary system, including excretion, elimination, homeostatic regulation, urine formation, and nephron anatomy. Learn how the urinary system maintains balance and removes waste from the body.

E N D
Chapter 26: The Urinary System BIO 211 Lecture Instructor: Dr. Gollwitzer
Today in class we will discuss: • The interrelationship between the CVS and urinary system • The major functions of the urinary system • Excretion • Elimination • Homeostatic regulation • The basic principles of urine formation • Major functions of each portion of the nephron and collecting system • The 3 basic processes involved in urine formation • Glomerular filtration • Filtration pressures • Tubular reabsorption • Tubular secretion
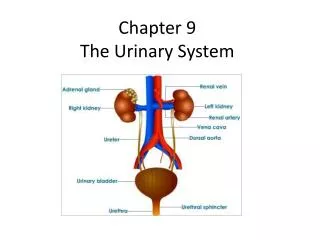
CVS and Urinary System • CVS delivers nutrients (from digestive tract) and O2 (from lungs) to cells in peripheral tissues • CVS carries CO2 and waste products from peripheral tissues to sites of excretion • CO2 removed at lungs • Most physiological waste products removed by urinary system
Major Functions of Urinary System • Excretion • Elimination • Homeostatic regulation of: • Blood plasma volume • Solute concentration
Major Functions of Urinary System • Excretion • Removal of organic wastes (e.g., urea, uric acid, creatinine) from body fluids (= urine formation) • Performed by kidneys which act as filtering units • Elimination • Discharge of waste products into environment (urination) • Occurs when urinary bladder contracts and forces urine through urethra and out of body
Major Functions of Urinary System: Homeostatic Regulation • Regulation of blood volume (water balance) and BP • Adjusts volume of water lost in urine • Releases • Renin • Involved in production of angiotensin II that affects BP, thirst, and other hormones (ADH, aldosterone) that affect water retention by kidneys • Erythropoietin • Stimulates erythropoiesis in bone marrow, maintains RBC volume
Major Functions of Urinary System: Homeostatic Regulation • Regulation of plasma ion concentrations (electrolyte balance) • Controls amounts lost in urine (e.g., Na+, K+, Cl-) • Controls Ca2+ levels by synthesis of calcitriol • Reabsorption (conservation) of valuable nutrients • Recycles valuable nutrients • e.g., amino acids, glucose • Prevents excretion in urine
Major Functions of Urinary System: Homeostatic Regulation • Stabilization of blood pH (acid-base balance) • Controls loss of H+ and HCO3- in urine • Detoxification • Of poisons, e.g., drugs • Deamination • Removes NH2 (amino group) so amino acids can be metabolized
Basic Principles of Urine Formation • Urine = fluid containing: • Water • Ions • Soluble compounds • Goal of urine production • To maintain homeostasis • By regulating volume and composition of blood
Basic Principles of Urine Formation • Involves excretion of solutes (i.e., metabolic/organic waste products) • Urea • Most abundant • Produced by breakdown of amino acids • Creatinine • Generated in skeletal muscle by breakdown of creatine phosphate (CP, high energy compound that plays a role as energy source in muscle contraction) • Uric acid • Formed by recycling nitrogenous bases from RNA
Basic Principles of Urine Formation • Waste products dissolved in bloodstream can only be eliminated when dissolved in urine • Thus removal accompanied by unavoidable water loss • To avoid dehydration, kidneys concentrate filtrate (i.e., reabsorb water) produced by glomerular filtration
Functional Anatomy of Nephron and Collecting System Figure 26–6
3 Processes Involved in Urine Formation • Glomerular filtration • Forces water and solutes out of blood in glomerulus into capsular space • filtrate • Tubular reabsorption • Recovers useful materials from filtrate • Tubular secretion • Ejects waste products, toxins, and other undesirable solutes into tubules
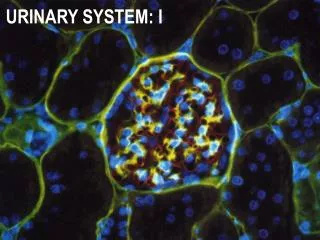
Glomerular Filtration • Occurs in renal corpuscle • Hydrostatic pressure forces water and solutes: • Out of blood in glomerulus • Into capsular space filtrate • Occurs solely on basis of size • Small solute molecules carried with filtrate
Glomerular Filtration • Involves passage across filtration membrane which is composed of 3 cellular units • Glomerular capillary endothelium • Lamina densa • Filtration slits
Glomerular Filtration • Glomerular capillary endothelium • Filtered through pores in fenestrated capillaries • Least selective filter • Pores too small for RBCs to pass through • Large enough for plasma proteins
Renal Corpuscle Figure 26–8
Glomerular Filtration • Lamina densa • Basement membrane of glomerular capillaries • More selective filter • Blocks passage of large proteins • Only small polypeptides, nutrients, and ions can cross
Glomerular Filtration • Filtration slits • Gaps between pedicels of podocytes (visceral epithelium around glomerulus) • Finest filter • No polypeptides pass through • Only nutrients, ions into capsular space • Thus, glomerular filtrate: • Does not contain plasma proteins or polypeptides • Does contain small organic molecules (e.g., nutrients) and ions in same concentration as in plasma
Filtration Pressures • Filtration pressure = balance between: • Hydrostatic (fluid) pressures • Glomerular hydrostatic pressure (GHP) in capillaries (50 mmg Hg) • Capsular hydrostatic pressure (CHP) (15 mm Hg) • Blood osmotic pressure (BOP) (25 mm Hg)
Filtration Pressures • Hydrostatic (fluid) pressures • Glomerular hydrostatic pressure (GHP) (50 mm Hg) • = BP in glomerular capillaries • Higher in glomerulus than in peripheral capillaries (35 mm Hg) • Because efferent arteriole smaller in diameter than afferent arteriole, need higher BP to force blood into it • Promotes filtration – pushes water and solutes out of plasma in capillaries into filtrate • Opposed by…
Filtration Pressures • Hydrostatic (fluid) pressures • Capsular hydrostatic pressure (CHP) (15 mm Hg) • Opposes filtration – pushes water and solutes out of filtrate into plasma in capillaries • Results from resistance to flow along nephron and conducting system that causes water to collect in Bowman’s capsule • More water in capsule more pressure
Filtration Pressures • Blood osmotic pressure (BOP) (25 mm Hg) • Results from presence of suspended proteins in blood • Promotes return of water into glomerulus • Opposes filtration • Tends to draw water out of filtrate and into plasma
Summary of Filtration Pressures • Hydrostatic pressures • GHP (pushing out of glomerulus) = 50 mm Hg • CHP (pushing into glomerulus) = 15 mm Hg • Net = 35 mm Hg (pushing out of glomerulus) • Osmotic pressure • BOP (draws into glomerulus) = 25 mm Hg • Filtration pressure = 10 mm Hg • Difference between net hydrostatic pressure and blood osmotic pressure
Summary of Filtration Pressures • Problems that affect filtration pressure • Can seriously disrupt kidney function • Can cause a variety of clinical symptoms, e.g., • Drop in systolic pressure from 120 to < 110 mm Hg would eliminate filtration pressure (10 mm Hg)
Today in class we will discuss: • The 3 basic processes involved in urine formation • Glomerular filtration • Glomerular Filtration Rate • Renal Failure • Tubular reabsorption • PCT, Loop of Henle & Countercurrent Exchange,DCT • Collecting System • Tubular secretion • PCT, DCT and Collecting system • Urine • Compare/contrast to plasma • General characteristics • Hormone influence of volume and concentration • Voluntary & involuntary regulation of urination and the micturition reflex
Glomerular Filtration Rate (GFR) • Gomerular filtration • Vital first step essential to all other kidney functions • Must occur so: • Waste products excreted • pH controlled • Blood volume maintained • GFR = amount of filtrate kidneys produce per minute • Avg GFR = 125 mL/min or 50 gal/day (out of 480 gallons of blood flow/day) • 10% of fluid delivered by renal arteries enters capsular spaces • 99% of this reabsorbed so urinate only 0.5 gallons/day
Glomerular Filtration Rate (GFR) • Measured using creatinine clearance test (CCT) • Breakdown of CP in muscle creatinine • Creatinine enters filtrate at glomerulus and is not reabsorbed so is excreted in urine • Can compare amount of creatinine in blood vs. in urine during 24 hour and estimate GFR • If glomerulus damaged, GFR will be altered (have more or less creatinine in urine than normal)
Glomerular Filtration Rate (GFR) • GFR depends on: • Adequate blood flow to glomerulus • Maintenance of normal filtration pressures • Affected by anything that reduces renal blood flow or BP, e.g., • Hypotension, hemorrhage, shock, dehydration • Decreased renal blood volume and/or BP decreased filtration pressure decreased GFR
Control of GFR • GFR increased by: • EPO (relatively minor) • Renin-angiotensin system • Natriuretic peptides (ANP and BNP)
Control of GFR • Decreased BP and/or blood volume • Decreased O2 JGA EPO • Increased RBCs • Increased O2 delivery • Increased blood volume increased BP • Increased filtration pressure • Increased GFR • Decreased renal blood flow JGA renin-angiotensin system • Increased blood volume increased BP • Increased filtration pressure • Increased GFR
EPO and Renin Figure 18–19b
Renin-Angiotensin System • Renin (enzyme) (prohormone) angiotensinogen (hormone) angiotensin I (in liver) • Angiotensin I angiotensin II (in lung capillaries) • Angiotensin II increased blood volume and BP increased GFR
Primary Effects of Angiotensin II • Stimulates constriction of efferent arterioles increased glomerular pressure • Directly stimulates reabsorption of Na+ and H2O in DCT increased blood volume and BP • Stimulates adrenal cortex aldosterone reabsorption of Na+ (and H2O) increased blood volume and BP • Stimulates posterior pituitary ADH reabsorption of H2O increased blood volume and BP • Stimulates thirst increased blood volume and BP • Stimulates vasoconstriction of arterioles
Renin-Angiotensin System: Response to Reduction in GFR Figure 26–11-0
Control of GFR • Increased blood volume or BP stretched cardiac muscle cells natriuretic peptides • ANP = atrial NP • BNP = brain NP (produced by ventricles) • Natriuretic peptides • Increase GFR • Decrease blood volume and BP • Via 2 mechanisms
Natriuretic Peptides Increase GFR • Act opposite to angiotensin II • Increase Na+ and H2O loss • Inhibit renin release • Inhibit secretion of aldosterone and ADH • Suppress thirst • Prevent increased BP by angiotensin II and NE • Increase glomerular pressures • Dilate afferent arterioles • Constrict efferent arterioles • Also increase tubular reabsorption of Na+ • Decreases blood volume and BP
Renal Failure • When filtration (GFR) slows, urine production decreases • Symptoms appear because water, ions, and metabolic wastes retained rather than excreted • Almost all systems affected: fluid balance, pH, muscular contraction, neural function, digestive function, metabolism • Leads to: • Hypertension (due to blood “backing up”) • Anemia due to lack of erythropoietin production • CNS problems (sleepiness, seizures, delirium, coma, death)
Renal Failure • Acute renal failure • From exposure to toxic drugs, renal ischemia, urinary obstruction, trauma • Develops quickly, but usually temporary • With supportive treatment can survive • Chronic renal failure • Condition deteriorates gradually • Cannot be reversed • Dialysis or kidney transplant may prolong life
Reabsorption and Secretion • Occur in all segments of renal tubules • Relative importance changes from segment to segment
Tubular Reabsorption • Molecules move from filtrate across tubular epithelium into peritubular interstitial fluid and blood • Water, valuable solutes (e.g., nutrients, proteins, amino acids, glucose) • Occurs through diffusion, osmosis (H2O), active transport by carrier proteins • Occurs primarily along PCT (also along renal tubule and collecting system)
Tubular Secretion • Molecules move from peritubular fluid into tubular fluid • Lowers plasma concentration of undesirable materials • Necessary because filtration does not force all solutes out of plasma • Primary method of excretion for many drugs • Occurs primarily at PCT and DCT
Reabsorption and Secretion: PCT • Primarily reabsorption • 60-70% of filtrate • Includes: • Organic nutrients (99-100%), e.g., glucose, amino acids, proteins, lipids, vitamins • Water (60-70%) • Ions (60-70%), e.g., Na+, Cl-; also K+, Ca2+, HCO3- • Reabsorbed materials enter peritubular fluid and capillaries • Secretion • H+, NH4+, creatinine, drugs, toxins
Reabsorption: Loop of Henle • Reabsorption • Na+, Cl- • Water • Accomplished by countercurrent exchange • Refers to exchange by tubular fluids moving in opposite directions • Fluid in descending limb flows toward renal pelvis • Fluid in ascending limb flows toward cortex
Countercurrent Exchange • Occurs because of different permeabilities of segments of LOH • Descending limb (thin) • Permeable to water • Relatively impermeable to solutes • Ascending limb (thick) • Relatively impermeable to water and solutes • Has active transport mechanisms • Pump Na+ and Cl- from tubular fluid into peritubular fluid
Countercurrent Exchange • Na+ and Cl- pumped out of thick ascending limb into peritubular fluid • Increases osmotic concentration in peritubular fluid around thin descending limb • Results in osmotic flow of H2O out of thin descending limb into peritubular fluid increased solute concentration in thin descending limb • Arrival of concentrated solution in thick ascending limb increases transport of Na+ and Cl- into peritubular fluid
Overview of Urine Formation Figure 26–16
Reabsorption and Secretion: DCT • Reabsorption (by vasa recta) • Na+ (under influence of aldosterone), Cl- • Ca2+(under influence of PTH and calcitriol) • H2O (under influence of ADH) • Secretion • K+ (in exchange for Na+), H+ • NH4+ (from deamination; produces lactic acid, ketone bodies acidosis) • Creatinine, drugs, toxins