POLIO VIRUS
POLIO VIRUS. ODUCHE EBUKA EDWIN. SYNOPSIS. Introduction Replicative cycle Transmission Epidermiology Pathogenesis Immunity Clinical findings Lab diagnosis Prevention and treatment. INTRODUCTION.

POLIO VIRUS
E N D
Presentation Transcript
POLIO VIRUS ODUCHE EBUKA EDWIN
SYNOPSIS • Introduction • Replicative cycle • Transmission • Epidermiology • Pathogenesis • Immunity • Clinical findings • Lab diagnosis • Prevention and treatment
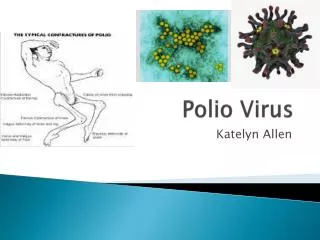
INTRODUCTION Poliovirus, the causative agent of poliomyelitis, is a human enterovirus and member of the family of Picornaviridae. Poliovirus is composed of an RNA genome and a protein capsid. Because of its short genome and its simple composition (only RNA and a non-enveloped protein coat) poliovirus is widely regarded as the simplest significant virus.
Poliovirus was first isolated in 1909 by Karl Landsteiner and his assistant Erwin Popper. In 1981, the poliovirus genome was published by two different teams of researchers: by Vincent Racaniello and David Baltimore atMIT and byNaomiKitamur and EckardWimmer at Stony Brook University
REPLICATIVE CYCLE • Poliovirus infects human cells by binding to animmunoglobulin-like receptor, CD155, (also known as thepoliovirus receptor (PVR) on the cell surface.Interactionof poliovirus and CD155 facilitates an irreversible conformational change of the viral particle necessary for viral entry. The virus is taken up by receptor-mediated endocytosis.
On entry the virus hijacks the cell's translation machinery; causing inhibition of cellular protein synthesis in favor of virus–specific protein production. Unlike the host cell's mRNAs the 5' end of poliovirus RNA is extremely long—over 700 nucleotides—and is highly structured. This region of the viral genome is called internal ribosome entry site(IRES) and it directs translation of the viral RNA. Genetic mutations in this region prevent viral protein production.
Poliovirus mRNA is translated as one long polypeptide. This polypeptide is then auto-cleaved by internal proteases into approximately 10 individual viral proteins, including • 3Dpol, an RNA dependent RNA polymerase whose function is to copy and multiply the viral RNA genome
2Apro and 3Cpro/3CDpro, proteases which cleave the viral polypeptide. • VPg (3B), a small protein that binds viral RNA and is necessary for synthesis of viral positive and negative strand RNA. • 2BC, 2B, 2C, 3AB, 3A, 3B proteins which comprise the protein complex needed for virus replication.
VP0, which is further cleaved into VP2 and VP4, VP1 and VP3 proteins of the viral capsid. next he assembly of new virus particles, (i.e. the packaging of progeny genome into a capsid) fully assembled poliovirus leaves the confines of its host cell 4 to 6 hours following initiation of infection in cultured mammalian cells.Themechanism of viral release from the cell is unclear, but each dying cell can release up to 10,000 polio virions.
TRANSMISSION Poliomyelitis is highly contagious via the fecal oral (intestinal source) and the oral-oral(oropharyngealsource) routes. The disease is transmitted primarily via thefecal-oral route, by ingesting contaminated food or water. It is occasionally transmitted via the oral-oral route,amode especially visible in areas with good sanitation and hygiene. Polio is most infectious between seven and 10 days before and after the appearance of symptoms, but transmission is possible as long as the virus remains in the saliva or feces
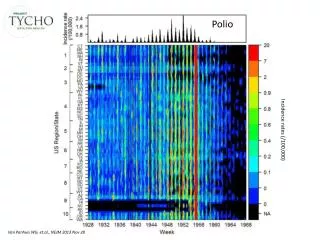
EPIDERMIOLOGY • Polio has been successfully eradicated from the western world, but its still endemic in Pakistan and Nigeria. The successful eradication in the western world is due to the widespread of polio vaccine • A global effort to eradicate polio began in 1988, led by the World Health Organization, UNICEF, and The Rotary Foundation. These efforts have reduced the number of annual diagnosed cases by 99%; from an estimated 350,000 cases in 1988 to a low of 483 cases in 2001
In 2012, cases decreased to 223. Polio is one of only two diseases currently the subject of a global eradication program, the other being Guinea worm disease. So far, the only diseases completely eradicated by humankind aresmallpox, which happened in 1979 and rinderpest in 2010. • As of 2013, polio remains endemic in only three countries: Nigeria, Pakistan, and Afghanistan
On 27 March 2014, World Health Organization(WHO) declared India a polio free country with no case of disease being reported in last three years. • In 2003 in northern Nigeria—a country which at that time was considered provisionally polio free—a fatwa was issued declaring that the polio vaccine was a conspiracy by the United States and the United Nations against the Muslim faith, saying also that the drops were designed to sterilize the true believers. Subsequently, polio reappeared in Nigeria and spread from there to several other countries.Healthworkers administering polio vaccine have been targeted and killed by gunmen on motorcycles in Kano
PATHOGENESIS • Poliovirus is an enterovirus. Infection occurs via the fecal–oral route, meaning that one ingests the virus and viral replication occurs in the alimentary tract. Virus is shed in the feces of infected individuals. In 95% of cases only a primary, transient presence of viremia (virus in the bloodstream) occurs, and the poliovirus infection is asymptomatic. In about 5% of cases, the virus spreads and replicates in other sites such as brown fat, reticuloendothelial tissue, and muscle. The sustained viral replication causes secondary viremia and leads to the development of minor symptoms such as fever, headache and sore throat.
Paralytic poliomyelitis occurs in less than 1% of poliovirus infections. Paralytic disease occurs when the virus enters the central nervous system (CNS) and replicates in motor neurons within the spinal cord, brain stem, or motor cortex, resulting in the selective destruction of motor neurons leading to temporary or permanentparalysis. In rare cases, paralytic poliomyelitis leads to respiratory arrest and death. In cases of paralytic disease, muscle pain and spasms are frequently observed prior to onset of weakness and paralysis. Paralysis typically persists anywhere from days to weeks prior to recovery. Poliomyelitis is a disease of the central nervous system. However, CD155 is believed to be present on the surface of most or all human cells.
IMMUNITY • Polio virus can evade the immune system in 2 ways • It replicates very fast and will overwhelm the host organ before an immune response is mounted • Secondly it is capable of surviving the highly acidic nature of the GIT allowing the virus to infect the host and spread through the lymphatic systems to other parts of the body
Individuals who are exposed to poliovirus, either through infection or by immunization with polio vaccine, developimmunity. In immune individuals, antibodies against poliovirus are present in the tonsils and gastrointestinal tract (specifically IgA antibodies) and are able to block poliovirus replication; IgG and IgM antibodies against poliovirus can prevent the spread of the virus to motor neurons of the central nervous system. Infection with one serotype of poliovirus does not provide immunity against the other serotypes, however second attacks within the same individual are extremely rare.
CLINICAL FINDINGS • Although polio can lead to paralysis and death, most people who have polio are asymptomatic and are unaware of the virus • Nonparalytic polio • Some people who develop symptoms from the poliovirus contract nonparalytic polio — a type of polio that doesn't lead to paralysis (abortive polio). This usually causes the same mild, flu-like signs and symptoms typical of other viral illnesses. • Signs and symptoms, which generally last one to 10 days, include: • Fever
Sore throat • Headache • Vomiting • Fatigue • Back pain or stiffness • Neck pain or stiffness • Pain or stiffness in the arms or legs • Muscle weakness or tenderness • Meningitis
Paralytic polio • In rare cases, poliovirus infection leads to paralytic polio, the most serious form of the disease. Paralytic polio has several types, based on the part of your body that's affected — your spinal cord (spinal polio), your brainstem (bulbar polio) or both (bulbospinal polio). • Initial signs and symptoms of paralytic polio, such as fever and headache, often mimic those of nonparalytic polio. Within a week, however, signs and symptoms specific to paralytic polio appear, including: • Loss of reflexes • Severe muscle aches or weakness • Loose and floppy limbs (flaccid paralysis), often worse on one side of the body
PARALYTIC POLIOMYELITIES • This is the most feared manifestation of polio virus, the viral infection destroys the presynaptic motor neuron in the anterior horn of the spinal cord as well as the post synaptic neuron leaving the horn. • NOTE- no sensory loss
Post-polio syndrome • Post-polio syndrome is a cluster of disabling signs and symptoms that affect some people several years — an average of 35 years — after they had polio. Common signs and symptoms include: • Progressive muscle or joint weakness and pain • General fatigue and exhaustion after minimal activity • Muscle atrophy • Breathing or swallowing problems • Sleep-related breathing disorders, such as sleep apnea • Decreased tolerance of cold temperatures • Cognitive problems, such as concentration and memory difficulties • Depression or mood swings
LAB DIAGNOSIS • A laboratory diagnosis is usually made based on recovery of poliovirus from a stool sample or a swab of the pharynx.Antibodies to poliovirus can be diagnostic, and are generally detected in the blood of infected patients early in the course of infection. Analysis of the patient's cerebrospinal fluid (CSF), which is collected by alumbar puncture ("spinal tap"), reveals an increased number of white blood cells (primarily lymphocytes) and a mildly elevated protein level. Detection of virus in the CSF is diagnostic of paralytic polio, but rarely occurs.
TREATMENT AND PREVENTION • There is no cure for polio. The focus of modern treatment has been on providing relief of symptoms, speeding recovery and preventing complications. Supportive measures include antibiotics to prevent infections in weakened muscles, analgesics for pain, moderate exercise and a nutritious diet. Treatment of polio often requires long-term rehabilitation, including occupational therapy, physical therapy, braces, corrective shoes and, in some cases, orthopedic surgery.]
Other treatments for polio include hydrotherapy, electrotherapy, massage and passive motion exercises, and surgical treatments, such as tendon lengthening and nerve grafting.
Inactivated Polio Vaccine This vaccine was developed by Jonas Salk, it contains formalin killed viruses that are injected subcuteanously, proving and igG response that will prevent future viremia This is the vaccine used in the US and other developed countries
Oral polio vaccine • This was developed by Albert Sabin. This contains attenuated polio virus that has lost its ability to multiply in the CNS. It is taken orally and shed in faeces and doesn’t cause paralytic poliomyelitis. • The oral vaccine not only allows formation of igG in the blood, it also allows formation of igA in the GIT. • This vaccine can cause Vaccine-associated paralytic poliomyelitis
REFERENCES • "ICTV 2009 Master Species List Version 10". International Committee on Taxonomy of Viruses. August 2011. • Ryan KJ, Ray CG, ed. (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. ISBN 0-8385-8529-9. • HogleJ (2002). "Poliovirus cell entry: common structural themes in viral cell entry pathways".Annu Rev Microbiol56: 677–702.doi:10.1146/annurev.micro.56.012302.160757.PMC 1500891. PMID 12142481. • GoodsellDS (1998). The machinery of life. New York: Copernicus. ISBN 0-387-98273-6. • Paul JR (1971). A History of Poliomyelitis. (Yale studies in the history of science and medicine). New Haven, Conn: Yale University Press. ISBN 0-300-01324-8.
Racanielloand Baltimore; Baltimore, D (1981)."Molecular cloning of poliovirus cDNA and determination of the complete nucleotide sequence of the viral genome". Proc. Natl. Acad. Sci. U.S.A.78(8): 4887–91. doi:10.1073/pnas.78.8.4887.PMC 320284. PMID 6272282. • Kitamura N, Semler B, Rothberg P, et al. (1981). "Primary structure, gene organization and polypeptide expression of poliovirus RNA". Nature291 (5816): 547–53. doi:10.1038/291547a0. PMID 6264310. • De Jesus NH (2007). "Epidemics to eradication: the modern history of poliomyelitis". Virol. J.4 (1): 70. doi:10.1186/1743-422X-4-70. PMC 1947962.PMID 17623069.