PID
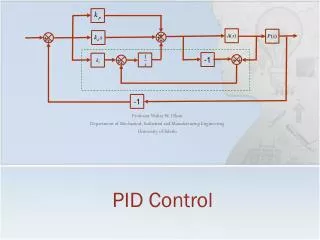
PID. Ascending infection of the upper female genital tract and includes Endometritis Salpingo-oophritis Pelvic peritonitis Parametritis Perihepatitis. PID. Lactobacilli Diphtheroids Staph. Epidermidis Strep. Fecalis GBS E.Coli C. Albicans. Vaginal flora. Grade 1 (Normal).


PID
E N D
Presentation Transcript
Ascending infection of the upper female genital tract and includes Endometritis Salpingo-oophritis Pelvic peritonitis Parametritis Perihepatitis PID
Lactobacilli Diphtheroids Staph. Epidermidis Strep. Fecalis GBS E.Coli C. Albicans Vaginal flora Grade 1 (Normal) Grade III (Vaginosis) • G. Vaginalis • B. Fragilis • M. Hominis • Peptococci • Cl. Welchii • Listeria
Microbiology of PID STD N. gonorrhoea C. trachomatis Endogenous Pathogens G. Vaginalis E. coli Anaerobic streptococci B. Fragilis M. Hominis Respiratory Pathogens H.Influenza Strep. Pyogenes Pneumococci
Menstruation Instrumentation Sperm transport IUCD How does the organism overcome the genital barrier?
Adolescent PID Westrom in 1980 gave the following figures in sexually active adolescent girls Age in years Risk of PID 15 1/8 16 1/10 24 1/80 • Why the incidence is high? • Sexual activity • Cervical ectopy • Poor sex education
Enhancing Factors Inhibitory Factors Cervicitis Cervical mucus N. gonorrhoea Bactericidal antibodies C. trachomatis Oral contraceptives Endometritis Bacterial vaginosis Douching Intrauterine device Factors That Enhance or Inhibit the Development of Acute Salpingitis
Sexual PID Sexual activity Sexual partners Sex During menses Orogenital sex Non-sexual PID Instrumentation Pregnancy termination IUD-related Douching Risk factors
Difficulty of estimation Silent PID Atypical PID No confirmatory Lap. 3% of women have PID during their lifetime It is more in adolescents, blacks and prostitutes Risk of recurrence is 25% Incidence of PID
Essential criteria Tender lower abdomen Tender tubal points Cervical motion tenderness Manifestations of PID Additional criteria • Fever > 38.30C (PO) • Mucopurulent cervicitis • Lab • ESR > 40 mm/hr • CRP > 5 mg% • Leucocytosis > 104/l • Positive smear • Positive culture • Serodiagnosis Elaborate criteria • Plasma cell endometritis • Sonography • X-ray • Culdocentesis • Lap.
Spontaneous abortion Appendicitis Ectopic pregnancy Ruptured ovarian cyst Degenerating myoma Endometriosis IBD Diverticulitis Differential diagnosis of PID
Silent PID Recurrent PID Fitz-Hugh-Curtis syndrome Atypical PID
No clinical manifestations Tubal infertility Antibody to chlamydia trachomatis Silent PIDthree times manifest PID
Infertility Ectopic pregnancy Pelvic pain Hydrosalpinx Pyosalpinx Tubo-ovarian abscess Pelvic abscess Pelvic adhesion Long-term sequelae of PID
Recovery Tubal deciliation Tubal occlusion Pelvic abscess Pelvic adhesion Fate of tubal infection
Tuberculosis Actinomycosis Schistosomiasis Chronic PID
Sex education Barrier contraceptives Antibiotic for high risks, HSG, IUCD Aggressive treatment Prevention of PID
Poor patient compliance Severe clinical disease Suspected anaerobiosis Uncertain diagnosis Indications for hospitalization
Bed rest (Fowler position) Avoidance of sex Treatment of male partner Screen for STD Any patient with fever and abdominal pain is not given antibiotic unless the diagnosis is certain or laparotomy is decided General advice
Uncertain diagnosis Poor responders Recurrent case Indications for laparoscopy
Parenteral versus oral therapy Monotherapy versus multiple ones Before versus after microbial diagnosis Antibiotic therapy
Inpatient regimen Regimen 1 Mefoxin 2g IV/6hr 1w doxycycline 100 mg bid 2 w Regimen II Dalacin 0.9 g IV/8hr 1w Garamycin 60 mg/8hr 1 w doxycycline 100 mg bid 2 w Outpatient regimen Regimen 1 Mefoxin 2g IM doxycycline 100 mg bid 2 w Regimen II Amoxicillin 3g PO (Probenecid) doxycycline 100 mg bid 2 w Antibiotic therapy
Question the diagnosis of PID Causes of failure Capsule that protects from phagocytosis L-form of bacteria B-lactamase production Failure of antibiotic therapy
Fertility Surgery????? Pelvic Clearance