Download

1 / 27
480 likes | 1.55k Vues
Monoamine Oxidase Inhibitors. By Dr. Yieldez Bassiouni Professor of Pharmacology. Monoamine oxidase inhibitors.

E N D
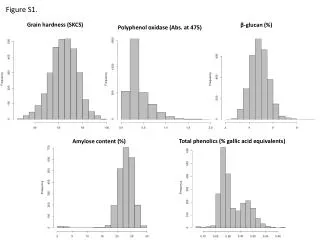
Monoamine Oxidase Inhibitors By Dr. YieldezBassiouni Professor of Pharmacology
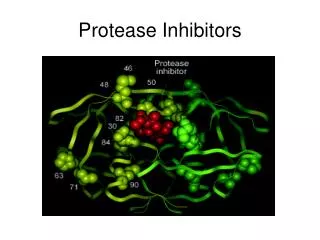
Monoamine oxidase inhibitors • Monoamine Oxidase Inhibitors (MAOIs) are a class of powerful antidepressant drugs. They are particularly effective in treating atypical depression, panic disorders, social phobia • Due to potentially lethal dietary and drug interactions, MAOIs had been reserved as a last line of Rx, used only when other classes of antidepressant drugs (e.g. SSRIs and TCAs) have failed
What is Monoamine Oxidase? • MAO is a mitochondrial enzyme found in most tissues; NS, liver, gut (presynaptic nerves). • The enzyme is responsible for the degradation of monoamine neurotransmitters • There are two forms of monoamine oxidase; MAO-A and MAO-B • MAO-A is responsible for NE, 5-HT & tyramine metabolism • MAO-B is more selective for dopamine metabolism
Mechanism of action • MAOIsact by inhibiting the activity of MAO thus preventing the breakdown of monoamine neurotransmitters and thereby increasing their availability in the synaptic cleft
The early MAOIs inhibited MAO irreversibly.i.e they permanently deactivate it, and the enzyme cannot function until it has been replaced by the body, which can take about two weeks. • A few newer MAOIs, moclobemide, are reversible, they are able to detach from the enzyme.
Classification of MAOIs According to Reversibility, MAOIs can be classified into: 1-Irreversible agents; Tranylcypromine, phenelzineirreversibly combine with the enzyme & have a prolonged action 2- Reversible agents; - Moclobemide.
Classification of MAOIs According to selectivity, MAOIs can be classified into: 1-Non selective agents; Phenelzine,Tranylcypromine They inhibit MAO A, MAO B 2- Selective agents; -Moclobemide, (MAO-A)I -Selegiline, (MAO-B)I .
MAOIs approved to treat depression • Phenelzine • Tranylcypromine • Moclobemide • Selegiline
Hypertensive Crisis • Many foods containing tyramine is normally degraded in the gut by MAO-A • Since the enzyme is inhibited by MAOIs, tyramine from ingested food is absorbed, and then taken up into adrenergic neurons. • It is converted into octopamine - a false transmitter which causes massive release of NE and may result in hypertensive crisis -.
Food interaction • People taking MAOI’s should avoid foods rich in tyramine • e.g.aged wine , aged cheese, liver, sausages, fish • Some meat and yeast extracts
Drug Interactions 1-The use of MAO inhibitors with TCAs causes elevated levels of NE and hypertensive crisis 2-Concurrent use of a MAOI and fluoxetine may lead to the serotonin syndrome
Drug Interactions 3-Local anaestheticsor cold medications contain (pseudoephedrine, ephedrine) have synergistic effects with the increased levels of catecholamines caused by MAOIs 5-MAOIs with pethidine may lead to abnormal syndrome characterized by hyperpyrexia, irritability, hypotension and coma due to an abnormal pethidine metabolite resulting from the inhibition of the normal demethylation pathway of pethidine by MAOIs
Current use of MAOIs • They are not the first-line drugs because of the great drug interaction risks & the complicated dietary restrictions required • The reversible selective MAO-A inhibitor moclobemide & the selective MAO-B inhibitor selegilinehave a greater safety margin • Newer MAOIs are used for the treatment of atypical depression ( + severe anxiety or panic attacks, marked obesity) and depression resistant to therapy
Selegiline Patch (Emsam™) • Selective MAO-B Inhibitor • Bioavailability Orally: 4% Transdermally: 74% • Avoid first pass GI exposure • Much less inhibition of gut & liver MAO-A
Mixed - Action & Atypical Antidepressants
Mixed-Action Antidepressants • Selective serotonin- norepinephrine reuptake inhibitors ( SNRIs) • Norepinephrine reuptake inhibitors (NRIs) • Norepinephrine-dopamine reuptake inhibitors (NDRIs)
Serotonin-norepinephrine reuptake inhibitors (SNRIs) • SNRIs are a newer form of anti-depressants that work on both 5-HT (SSRI-plus)and weak NE reuptake blockade • They have similar side effects to the SSRIs except increased risk of hypertension • Examples : Venlafaxine
Venlafaxine • Potent inhibitor of serotonin, NE reuptake transporter (SNRIs) • Unlike, TCAs, has little activity at adrenergic, histaminic and muscarinic receptors (fewer side effects than TCAs)
Reboxetine • Nareuptake inhibitor [ NARIs ] • No affinity for 5HT, DA, H, muscarinic receptors
Reboxetine • Has a positive effect on the concentration and motivation in particular • Safe to combine with SSRIs • Minimal side effects only related to activation of adrenergic system as tremor, tachycardia
Mirtazapine • Belongs to a newer class of antidepressants • acts by blocking presynaptic central alpha-2 adrenergic receptors leading to increased release of NE and serotonin • + blocking serotonin receptors (5HT3 , 5HT2 receptors)------- > lower incidence of adverse effects such as anxiety, insomnia, and nausea • has only minimal activity at dopaminergic and muscarinic receptors.
Mirtazapine • Does not cause anti-muscarinic side effects , less sexual dysfunction • Side effects include sedation (antihistaminic effect) and weight gain
Mirtazapine is preferred in cancer patients because: • Improves appetite • nausea & vomiting ( 5-HT3 blocking) • body weight • Sedation (antihistaminic) • Less sexual dysfunction (5-HT2 blocking) • Has no anti-muscarinic effect
Norepinephrine-dopamine reuptake inhibitors (NDRIs) • Bupropion (Wellbutrin ) is a unique drug that has been shown to possess significant potency as NE and dopamine reuptake inhibitor in the brain with no direct action on the serotonin system
Therapeutic uses: 1- Treatment of major depression and bipolar depression 2-Can be used in smoking cessation as it reduces the severity of nicotine craving & withdrawal symptoms Advantages: • No sexual dysfunction • No weight gain (as no serotonin effect) • No orthostatic hypotension Side effects:ppt seizures :it threshold of neuronal firing