Download
1 / 1
10 likes | 180 Vues
COMBINED LOW DOSE RATE BRACHYTHERAPY AND EXTERNAL BEAM RADIOTHERAPY RESULT IN A FAVORABLE URINARY SYMPTOM PROFILE RELATIVE TO BRACHTHERAPY MONOTHERAPY AT THE SAME BIOLOGICAL EQUIVALENT DOSE (BED). JAMIE A. CESARETTI, M.D., M.S.,* RICHARD G. STOCK, M.D.,* NELSON N. STONE, M.D., *†

E N D
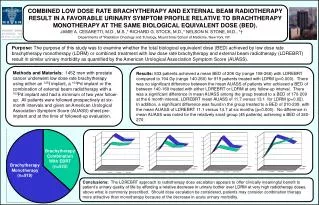
COMBINED LOW DOSE RATE BRACHYTHERAPY AND EXTERNAL BEAM RADIOTHERAPY RESULT IN A FAVORABLE URINARY SYMPTOM PROFILE RELATIVE TO BRACHTHERAPY MONOTHERAPY AT THE SAME BIOLOGICAL EQUIVALENT DOSE (BED). JAMIE A. CESARETTI, M.D., M.S.,* RICHARD G. STOCK, M.D.,* NELSON N. STONE, M.D., *† Departments of *Radiation Oncology and †Urology, Mount Sinai School of Medicine, New York, NY. Purpose: The purpose of this study was to examine whether the total biological equivalent dose (BED) achieved by low dose rate brachytherapy monotherapy (LDRM) or combined treatment with low dose rate brachytherapy and external beam radiotherapy (LDREBRT) result in similar urinary morbidity as quantified by the American Urological Association Symptom Score (AUASS). Methods and Materials: 1452 men with prostate cancer underwent low dose rate brachytherapy using either an 125I implant, a 103Pd implant or the combination of external beam radiotherapy with a 103Pd implant and had a minimum of two year follow-up. All patients were followed prospectively at six-month intervals and given an American Urological Association Symptom Score (AUASS) sheet pre-implant and at the time of followed-up evaluation. Results: 533 patients achieved a mean BED of 206 Gy (range 158-266) with LDREBRT compared to 194 Gy (range 140-260) for 919 patients treated with LDRM (p=0.000). There was no significant difference between the mean AUASS of patients who achieved a BED of between 140-169 treated with either LDREBRT or LDRM at any follow-up interval. There was a significant difference in mean AUASS among the group treated to a BED of 170-209 at the 6 month interval, LDREBRT mean AUASS of 11.7 versus 13.1 for LDRM (p=0.02). In addition, a significant difference was found in the group treated to a BED of 210-239, with the mean AUASS of LDREBRT 11.1 versus 14.7 at six months (p=0.000). No difference in mean AUASS was noted for the relatively small group (45 patients) achieving a BED of 240-270. Brachytherapy Combination With EBRT (n=533) Brachytherapy Monotherapy (n=919) Conclusions: The LDREBRT approach to radiotherapy dose escalation appears to offer clinically meaningful benefit to patient’s urinary quality of life by affording a relative decrease in urinary bother over LDRM at very high radiotherapy doses, above what is commonly prescribed. Should dose escalation be considered, patients may consider combination therapy more attractive than monotherapy because of the decrease in acute urinary morbidity.