Download
1 / 32
320 likes | 471 Vues
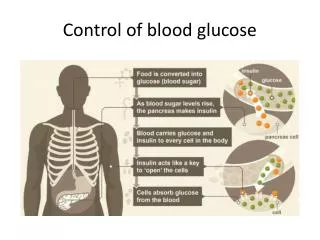
Blood Glucose Control in a Schizophrenic Population in an Outpatient Setting. Daniel Molloy, MD Mentor: James Stephen, MD. Schizophrenia. Complex psychiatric disorder with many medical and psychosocial complications.

E N D
Blood Glucose Control in a Schizophrenic Population in an Outpatient Setting Daniel Molloy, MD Mentor: James Stephen, MD
Schizophrenia • Complex psychiatric disorder with many medical and psychosocial complications. • Characterized by a heterogeneous mixture of clinical features psychosis (1). • Incidence: 10 to 40 / 100,000 population • High risk for poverty, unemployment, homelessness or inadequate housing, ill health, and poor access to health care(1). Meltzer H.Y., Bobo W.V., Heckers S.H., Fatemi H.S. (2008). Chapter 16. Schizophrenia. In M.H. Ebert, P.T. Loosen, B. Nurcombe, J.F. Leckman (Eds), CURRENT Diagnosis & Treatment: Psychiatry, 2e.
Background • Per DSM – IV TR (2), to diagnose schizophrenia, a patient must have at least 2 of the following: • Delusions • Hallucinations • Disorganized speech and/or • Disorganized behavior, • Negative symptoms (alogia, avolition, and flat affect). • These must be at least 6 months in duration and produce disturbances in work, self-care, and interpersonal relations. American Psychiatric Association. DSM-IV. Diagnostic and statistical manual of mental disorders. 4th ed. Washington: American Psychiatric Association, 1994: 273-315
Background Associated medical issues(3): • 20% decreased life expectancy • Increased rates of cardiovascular and metabolic abnormalities. • Overall poorer health – related quality of life . McGrath J, Saha S, Welham J, El Saadi O, Macauley C, Chant D. “ A systematic review of the incidence of schizophrenia: the distribution of rates and the influence of sex, urbanicity, migrant status and methodology.” BMC Med . 2:13 (2004).
Background • Prevalence of type 2 diabetes in schizophrenic populations can be 2–4 times higher than in the general population, 15–18%(4). • The exact reason in unclear, but likely to include • Poor diet • Sedentary lifestyle • Substance abuse • Family association - monozygotic twins/1st degree relatives ‘Schizophrenia and Diabetes 2003’ Expert Consensus Meeting, Dublin, 3–4 October 2003: consensus summary, The British Journal of Psychiatry (2004) 184: s112-s114.
Hemoglobin A1c • Formed by the irreversible, nonenzymatic binding of glucose to the terminal end of the beta chain of hemoglobin • Serves as a predictable measure of average blood glucose over period of 90 – 120 days. • ADA Clinical Practice Recommendations now recommend using HbA1c to diagnose diabetes using a NGSP-certified method and a cutoff of HbA1c ≥6.5%(5). Diabetes Care January 2012 vol. 35 no. Supplement 1 S11-S63
Hemoglobin A1c • Certain limitations to hemoglobin A1c are known: • Dependent on lifespan of RBC • Influenced by hemoglobin variety • Laboratory –dependent standardization
Antipsychotic medications • Antipsychotic medications commonly used in the treatment of schizophrenia have a well – documented tendency to cause hyperglycemia and/or insulin resistance (6). • Particularly pronounced in patients receiving certain members of the class of second – generation antipsychotics(6). • Cause is not entirely elucidated Gautam, S., and PS Meena. "Drug-emergent Metabolic Syndrome in Patients with Schizophrenia Receiving Atypical (second-generation) Antipsychotics." Indian Journal of Psychiatry 53.2 (2011): 128-33
Rationale • Quality outcome measurements are becoming an increasingly important aspect of day – to –day practice.
Rationale • Bias towards mentally ill patients influences healthcare provider decision making (4). • One study with standardized patient showed HCP less likely to prescribe appropriate therapies/medications to schizophrenic patients(4). • Also includes mental health professionals (4). Mittal, Dinesh, MD. "Does Serious Mental Illness Influence Treatment Decisions of Physicians and Nurses?" Lecture. American Psychiatric Assocation 2012 Annual Meeting. San Francisco. 20 May 2013. APA 166th Meeting. American Psychiatric Association, May 2013
Aims • Primary Objective: To determine whether a difference in average blood glucose control exists between a schizophrenic and a non - schizophrenic population in an outpatient setting.
Aims • Secondary Objectives: • To determine whether an association exists between A1c levels and the number of healthcare contact events during study period. • To assess the prevalence of vascular disease between schizophrenic and non – schizophrenic patients.
Methods • Retrospective case – control study • IRB approval obtained prior to study commencement • Data collected over a one year period from April 2012 to April 2013 • Chart – based; information obtained from EMR
Methods • Inclusion criteria: • Diagnosis of Schizophrenia • Treated in outpatient setting • At least one hemoglobin A1c obtained within the study period
Methods • Exclusion criteria: • End stage renal disease • Hemolytic anemia/ hemoglobinopathy • No hemoglobin A1c within study period
Methods 245 Schizophrenic patients identified. 72 diagnoses of Diabetes mellitus. 7 excluded due to exclusion criteria Total of 65 patients included
Methods • A control cohort of 65 randomly sampled diabetic patients was recruited based on several matching variables: • Age • Race • Gender.
Variables • Age • Gender • Race • BMI • LDL level • Triglyceride level • HDL level • Smoking status • Number of clinic visits during study period • Medications for schizophrenia • Use of Insulin therapy • Anemia • Kidney disease • Vascular complications
Statistical Analysis • ANCOVA, t-tests, chi-square (χ2) tests as appropriate. • SPSS software (SPSS Inc, Chicago, Illinois) was used for data analysis. • P<0.05 was considered significant
Schizophrenia and diabetes – associated vascular complications Vascular complications defined as coronary artery disease, peripheral vascular disease, and cerebrovascular disease
Hemoglobin A1c inSchizophrenic patients treated with typical vs Atypical Antipsychotics
Limitations of Study • Retrospective • Chart based • Multiple providers participating in patient care
Conclusions • There was a significant difference in the hemoglobin A1c between patients with schizophrenia {mean A1c 6.6, SD =1.3} and without schizophrenia {mean A1c 8.4, SD =2.6} after controlling the effect of age, race, gender, BMI, anemia and number of clinic visits (p <0.001).
Conclusions 2. There was a significant difference in the prevalence of vascular diseases between patients with schizophrenia {9.2%} and without schizophrenia {33.8%} after controlling the effect of age, race, gender, BMI, anemia and number of clinic visits (p <0.001).
Conclusions 3. There was no significant difference in the hemoglobin A1c between schizophrenic patients taking atypical antipsychotics {mean A1c 6.9, SD =1.1} and patients taking typical antipsychotics{ mean A1c =6.4, SD = 1.6} (p<0.323).
Conclusion/Discussion • A diagnosis of schizophrenia does not mean that a patient is incapable of managing their medical conditions. • Caretakers must be careful to avoid letting bias influence their decision – making. • Further prospective study may uncover reasons for this difference.
Acknowledgements • Srikrishna Varun Malayala, MBBS • Khalid J Qazi, MD, MACP • Henri Woodman, MD • Nikhil Satchidanand, PhD