Download
1 / 58
620 likes | 1.23k Vues
Valvular Regurgitation Sheldon Litwin, M.D. Normal heart valves have minimal leakage (back flow, insufficiency, regurgitation) when they close Significant valvular regurgitation causes the heart to do excess work (like walking up a sandy hill)

E N D
Valvular RegurgitationSheldon Litwin, M.D. • Normal heart valves have minimal leakage (back flow, insufficiency, regurgitation) when they close • Significant valvular regurgitation causes the heart to do excess work (like walking up a sandy hill) • Over time, significant regurgitation usually leads to cardiac enlargement and contractile dysfunction
Clinical goals in Valvular Disease • Make the diagnosis • Slow the disease progression • Prevent complications • Intervene at just the right time • Not too soon, not too late
Key Concept in Valve Regurgitation • Timing of intervention is tricky!! • Chamber enlargement and contractile dysfunction develop very gradually • Don’t subject your patient to risks before it it necessary • Fix the problem before damage becomes irreversible (may need to intervene before symptoms develop)
LA Mitral Valve Disease • Annulus • Leaflets • Chordae • Papillary muscles • LV
Acute MR: Etiology • Ischemia/MI • Posterolateral hypokinesis • Papillary muscle rupture • Ruptured chordae • Endocarditis • Systolic Anterior Motion (SAM) of mitral leaflet(s)
LA MV LV Ruptured Papillary Muscle Always causes acute, severe MR - a surgical emergency.
Acute MR: Pathophysiology • Flow from LV (high pressure) to LA (low pressure) LA pressure PCWP pulmonary edema • Low compliance atria transmits LV pressure more directly to pulmonary capillaries • “forward” stroke volume (low cardiac output)
Acute MR: Management • Vasodilators (if BP adequate) • Reduce afterload regurgitant volume forward volume • Inotropic agents if LV function • Antibiotics for SBE • Surgery (MVR)!!!!!
Chronic MR:Etiology • Degenerative • mitral annular calcification (MAC) • Myxomatous degeneration/MVP • LV dilatation • Anorexigenic drugs (phen-fen) • Healed endocarditis (IE or noninfectious) • Hypertrophic cardiomyopathy • Rheumatic
Mitral Valve Prolapse • “Syndrome” vs. disease • overdiagnosis • Myxomatous degeneration of leaflets & chordae (increased MMP activity) • SBE prophylaxis if significant MR present (> mild) • Early valve repair for severe MR
Nonvalvular causes of MR • May occur without structural abnormalities o f valve • Usually LV dilatation and remodeling with increased sphericity • Stretch of annulus and lateral displacement of papillary muscles may cause malcoaptation of the leaflets
Quantification of MR:size of jet on echo Mild-Moderate Mod-Severe
Quantitation of MR: Regurgitant Volume • < 20 ml = trace • 20-30 ml = mild • 30-50 ml = mod • > 50 ml = severe
Quantification of MR: PISA Proximal Isovelocity Surface Area: Method for calculating effective regurgitant orifice area (ERO) Flow through the “hole” must be the same as the flow proximal to the hole (similar to continuity equation for aortic valve area). LV < 0.2 cm2 = mild 0.2-0.4 cm2 = mod >0.4 cm2 = severe MV LA
PISA TEE: Severe MR The bigger the PISA, the bigger the hole
Mitral Regurgitation Grade Pulm vein flow pattern, vena contracta width, effective regurgitant orifice area, regurgitant volume, regurgitant fraction
Compensation in chronic mitral regurgitation • Left atrial dilatation ( compliance) • Smaller change in pressure with same regurgitant volume • LA & PCWP may stay normal for many years • LV enlargement (to allow for maintained stroke volume) • ’s wall stress
Afterload in MR • LV afterload (resistance to LV ejection) is reduced because the LA is a low pressure alternate pathway for ejection • LV chamber function (EF) should theoretically be greater than normal if myocardial contractility is preserved • Once EF is below normal, significant LV dysfunction exists and it is likely to get worse once the mitral valve is replaced
Complications of chronic MR • Atrial fibrillation • LV dilatation and systolic dysfunction • Passive pulmonary hypertension with RV dysfunction
Chronic Compensated MR Normal Acute MR 70 ml 95 ml 100 ml EDV 170 ml LA 15 mmHg LA 25 mmHg LA 10 mmHg EDV 150 ml EDV 240 ml 70 ml ESV 30 ml ESV 50 ml 95 ml ESV 50 ml Chronic Decompensated MR Chronic Compensated MR Acute MR 65 ml 70 ml 95 ml LA 25 mmHg LA 25mmHg LA 15 mmHg EDV 260 ml EDV 240 ml EDV 170 ml 85 ml ESV 110 ml 70 ml 95 ml ESV 30 ml ESV 50 ml
Medical management of MR • Afterload reduction, Rx of arterial HTN • Rx heart failure (if not surgical candidate) • SBE prophylaxis • Rheumatic fever prophylaxis • Rx of atrial fibrillation • Rx of ischemia
Surgical Rx of chronic MR • Valve replacement replaces one disease with another • Thrombosis, infection, pannus, degeneration • Valve repair is far preferable when technically feasible • Excision of prolapsing/flail segments (posterior leaflet) with placement of annuloplasty ring
Timing of surgery for MR • Old approach was to wait for symptoms, LV enlargement or systolic dysfunction (typically serial echoes were performed) • Problem: wait too long? • With low morbidity/mortality of repair and low need for reoperation, trend is to recommend early repair for severe MR, even in asymptomatic patients with normal LV function
Percent Survivors Mitral Stenosis Mitral Regurgitation Aortic Regurgitation Aortic Stenosis Years Since Diagnosis
Indications for surgery in chronic, nonischemic MR • Class I • Acute symptomatic MR in which repair is likely • NYHA Class II-IV symptoms with normal LV function (EF > 60%) and LVESD < 45 mm • Symptomatic or asymptomatic with mild LV dysfunction (EF 50-60%) and/or LVESD 50-55 mm • Symptomatic or asymptomatic with moderate LV dysfunction (EF 30-50%) and/or LVESD 50-55 mm
Prosthetic Mitral Valves Mechanical: bileaflet tilting disc
Tricuspid valve regurgitation: etiology • Pulmonary hypertension • RV enlargement (infarct, dysplasia) • Primary tricuspid disease • Infectious endocarditis • trauma • Carcinoid • Pacing wires/catheters • Ebstein's anomaly • Iatrogenic/bioptome
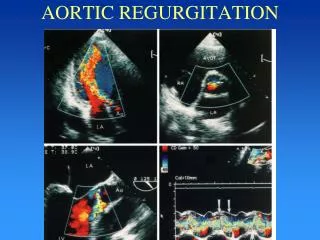
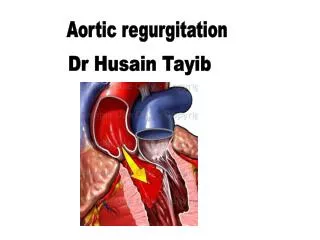
Aortic Insuffiency (regurgitation) • Valve normally open during systole, closed during diastole • AI occurs during diastole as aortic pressure is higher than LV pressure during this part of the cardiac cycle
Etiology of Aortic Valve Regurgitation • Annulus • Leaflets • Root
Ao AI Etiology: Aortic Root problems • Aortic root enlargement • Hypertension • Marfan’s syndrome • Syphillis • Aneurysm • Aortic dissection • Leaflet involvement • Shape of root/annulus • Ruptured sinus of Valsalva • Iatrogenic (septal myectomy)
AI Etiology: leaflet problems • Calcification/fibrosis • Degenerative • Rheumatic • Bicuspid • Endocarditis • Infectious • Noninfectious • Diet drugs
Quantification of AI:size of color jet on echo Mild-Moderate Mod-Severe Quantification is important because we usually only operate on patients with severe AI and it is necessary to track progression of disease
Quantification of AI • Pressure half time (Doppler) • The larger the hole in the valve, the faster pressure equilibrates between the aorta and the LV diastole • Short pressure half time indicates more severe AI (< 250 ms = severe) • Diastolic flow reversal in the descending aorta • Regurgitant volume (or fraction)
Severe AI Holodiastolic Flow Reversal in Descending Ao Arch & Descending Ao arch
AI Pathophysiology • Flow from Aorta (high pressure) to LV (low pressure) LVEDP LA pressure PCWP pulmonary edema • “forward” stroke volume (low cardiac output) • If AI occurs gradually, LV enlargement compensates and it is tolerated • If it happens suddenly, it typically causes pulmonary edema and/or shock
AI: signs • Large “forward” stroke volume to maintain actual stroke volume • Wide pulse pressure (e.g. 160/60) • Bounding peripheral pulses • Head bob • Uvula swinging • Quincke’s pulses (finger nails) • Etc.
Acute AI: Management • Vasodilators (if BP adequate) • Reduce afterload regurgitant volume forward volume • Inotropic agents if LV function • Antibiotics for SBE • Avoid intra-aortic balloon pump (makes AI worse) • Surgery (AVR)!!!!!
Chronic aortic insufficiency • LV enlargement to maintain forward stroke volume (’s wall stress) • LA & PCWP may stay normal for years • LV chamber function (EF) should be normal or greater than normal if myocardial contractility is preserved • Once EF is below normal, significant LV dysfunction exists and the outcome following valve replacement is worse
Timing of surgery for AI • Historical approach was to wait for symptoms, LV enlargement or systolic dysfunction (typically, serial echoes were performed) • Problem: wait too long? • As surgical techniques and prosthetic valves improve, earlier surgery may be warranted • However, aortic valve repair is not yet practical
Surgical Rx of chronic AI • Low EF increases mortality • Don’t wait too long
Medical management of AI • Afterload reduction (nifedipine, ACE inhibitors) - recent study suggests not helpful • Control arterial HTN • Treat heart failure (if not surgical candidate) • SBE prophylaxis • Rheumatic fever prophylaxis • All palliative