Basics of Raised Intracranial Pressure
460 likes | 804 Vues
Explore the fundamental principles of raised intracranial pressure including anatomy of the skull/spinal cord, CSF production/flow, causes, symptoms, and management. Learn about Monro Kellie Doctrine and cerebral perfusion pressure.

Basics of Raised Intracranial Pressure
E N D
Presentation Transcript
Raised Intracranial Pressure 03/05/12 Jeremy Kam Intern Royal Melbourne Hospital
Overview and Objectives • Basic Principles • Review Basic Anatomy of Skull and Spinal Cord • Review Basic Physiology of CSF production and flow • Monro Kellie Doctrine and concepts of CBF and CPP • Conceptualising ICP • Spectrum of Intracranial Pressure • Causes of Raised ICP • Assessment of Raised ICP • Symptoms • Signs and basic examination techniques • Investigating ICP • Management • Monitoring • Treatment
Contents of the Skull and the Monro Kellie Doctrine 1. Skull is a rigid box: The volume inside the cranium is a fixed volume (nearly). 2. The cranial contents incompressible (nearly) 3. The cranium and its constituents (blood, CSF, and brain tissue) create a state of volume equilibrium, such that any increase in volume of one of the cranial constituents must be compensated by a decrease in volume of another
Intracranial pressure “Intracranial pressure (ICP) is the pressure inside the skull and thus in the brain tissue and cerebrospinal fluid (CSF).” Constantly changing: exercise, coughing, straining, respiratory cycle
CEREBRAL PERFUSION PRESSURE CPP = MAP – ICP CEREBRAL PERFUSION PRESSURE = MEAN ARTERIAL PRESSURE – INTRACRANIAL PRESSURE Why do we care? • Brain survival depends on cerebral blood flow meeting cerebral metabolic requirements • Cerebral blood flow depends on Cerebral Perfusion Pressure • CPP depends upon ICP Normal CPP > 50 mmHg
INTRACRANIAL HYPERTENSION (finally) • What happens if ICP is too high? CPP = MAP – ICP • As ICP increases. Where MAP is constant. CPP will decrease. • Ideally CPP > 70-80mmHg • This is bad. • IC-HTN = ICP >20mmHg for >10 minutes • Increased ICP Decreased CPP Decreased CBF • MAP will compensate for awhile. CBF = CPP/CVR
Intracranial Hypertension • Why do we care? • Raised ICP may CAUSE problems itself e.g herniation, decrease in cerebral perfusion ischemia edema • Raised ICP may be a SIGN of problems being caused e.g mass effect; tumour, haemorrhage
SPECTRUM OF Raised ICP • ACUTE VS CHRONIC • SEVERE VS MILD • SYMPTOMS AND SIGNS from raised ICP • SYMPTOMS AND SIGNS from CAUSE of raised ICP • E.g: Acute Traumatic Intracranial Haemhorrhage Mass Effect Vs Neoplasm causing Mass effect
Intracranial Haemhorrages • Subdural Hematoma • Epidural Hematoma • Intracerebral Haemorrhage • Subarachnoid Haemorrhage • Cerebral Contusion
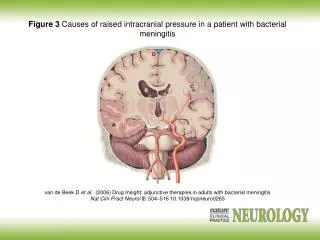
Space occupying Lesion Brain Abscess: • Develop as a result of a localizedbacterial cerebritis followed by necrosis and encapsulation • Mechanisms: • – Haematogenous • – Extension from neighbouring structures • – Penetrating injuries • Symptoms of infection may be absent in 50% of cases • Treatment: Excision drainage
Hydrocephalus 1 Obstructive hydrocephalus – obstruction from lesion along ventricle system. E.gtumor, colloid cyst, primary stenosis. 2 Communicating hydrocephalus- (a) obstruction to flow of CSF through the basal cisterns or (b) failure of absorption of CSF through the arachnoid granulations over the cerebral hemispheres. The most common causes of communicating hydrocephalus are infection (especially bacterial and tuberculous) and subarachnoid haemorrhage (either spontaneous, traumatic or postoperative). Treatment: Ventriculoperitoneal Shunt, 3rdVentriculostomy
Cerebral Oedema • Middle cerebral artery occlusion causing extensive infarction with mass effect. The appearances after decompressive craniotomy are shown in the third panel.
SYMPTOMS and Signs 1. Decreased LEVEL OF CONSCIOUSNESS - DROWSINESS • MOST IMPORTANT • never put down to simple sleepiness – measure Glasgow Coma Scale • Requires serial assessment Progressive decrease in GCS = worsening ICP state 2. Altered MENTAL STATUS • Confusion, restlessness, lethargy, difficulty thinking, 3. HEADACHE • Frontal, worse after lying down, Relieved by vomiting, Severe, Worse with coughing and straining 4. NAUSEA and VOMITING • Persistent 5. VISUAL CHANGES • Pupillary Dysfunction • Changes in Vision • VI nerve Palsy – false localising sign • Papilloedema - requires more than 24 hours
Papilloedema • Venous engorgement (usually the first signs) • loss of venous pulsation • hemorrhages over and / or adjacent to the optic disc • blurring of optic margins • elevation of optic disc • Paton's lines = radial retinal lines cascading from the optic disc
PROGRESSION OF SIGNS Continuous DECREASE in GCS stuporous comatose difficulty to arouse VISUAL CHANGES • Pupils become unilaterally enlarged progressing to fixed and dilated – eventually bilaterally fixed and dilated • Papilloedema NEUROLOGICAL FUNCTION • Decorticate or DecerebratePosturing • Loss of corneal and gag reflexes • Hemiplegia –that progresses VITAL SIGNS • Bradycardia • Increasing Hypertension – with widening pulse pressure • Irregular Respiration – neurogenic Hyperventilation • Respiratory arrest • Cushing's Triad • Hyperthermia SIGNS OF BRAIN HERNIATION
Cushing’s TRIAD seen in 33% of IC-HTN • HYPERTENSION (Widening Pulse Pressure) • BRADYCARDIA • RESPIRATORY IRREGULARITY INDICATES IMPENDING HERNIATION
BRAIN HERNIATION Syndromes • Transtentorial: • Foramen Magnum • Subfalcine
Severity and indications Indications for Treatment: ICP ≥ 20- 25 mmHg as the upper limit. Initiate Treatment for ICP > 20 mmHg – in combination with clinical exam and brain CT findings. Herniation can still occur at ICP < 20 Higher mortality and worse outcomes among patients with ICP persistently >20 compared to < 20. CPP Targets: Avoid CPP < 50mmHg Initiate treatment when CPP falls below 60mmHg
INVESTIGATIONS • LUMBAR PUNCTURE IS CONTRAINDICATED • CT Brain • MRI Brain • Biopsy • Angiography • Transcranial Doppler Flow Velocity
MANAGEMENT - MONITORING Indications for ICP Monitoring: • CT CRITERIA: • For salvageable patients with severe traumatic brain injury – GCS ≤ 8 after cardiopulmonary resuscitation • Abnormal admitting brain CT (60% risk of IC-HTN) or • Normal brain CT but with ≥2 risk factors (=60% risk of IC –HTN vs 13% r.f -ve): • Age >40 years • SBP < 90 mmHg • Decerebrate or decorticate posturing on motor exam – unilateral or bilateral • Neurological criteria – where GCS ≥ 9 – low risk for IC-HTN – serial neurological exam • Multiple system injury – where ICP likely to be effected by interventions e.g large volume IV fluids, PEEP • Traumatic IC Mass – EDH, SDH, depressed skull fracture • Post Op – may elect • Non-traumatic • Contraindications to ICP monitoring: “awake” patient, coagulopathy
INVASIVE ICP Monitoring • Intraventricular Catheter – IVC • Most accurate, allows therapeutic CSF drainage • May be difficult to insert into compressed or displaced ventricles, may obstruct • Intraparenchymal monitor • Subarachnoid Screw (bolt)
MANAGEMENT 1. MAINTAIN CEREBRAL PERFUSION PRESSURE by LOWERING ICP • Reduce size of brain VOLUME by decreasing cerebral volume, CSF fluid volume, or blood volume while maintaining cerebral perfusion • Make more SPACE – e.g surgical decompression • GOAL ICP <20 mmHg and CPP > 50mmHg 2.DECREASE METABOLIC DEMANDS 3. PREVENT COMPLICATIONS • GI risk of developing Cushing stress ulcers and GI bleeding. Give PPIs and H2 antag. • Fluid and electrolytes – diabetes inspidus - desmopressin. Close monitoring of electrolytes. • Hematological – DIC can occur after severe head injury. Coagulopathies aggressively treated FFP and Vit K 10mg a daily. • Nutrition 4. IDENTIFY CAUSE – TREAT • e.g remove space occupying lesions, insert VP shunt
BLOOD VOLUME ↓ ICP via ↑ Venous Outflow Elevation of Head of Bed 30-45 degrees • optimised trade off between promoting Venous Outflow vs Reducing MAP Keep Neck Straight Midline, avoid tight trach tape Maintain CPP with Normotension Avoid Hypotension (SBP < 90 mm Hg) Achieved via normalising intravascular volume. Use of pressors if needed. Control hypertension if present, Nitroprusside if nil tachyvs beta blocker if tachy Hyperventilation May be necessary for brief periods when acute neurologic deterioration. Do not use prophylactically. Short term. • Ventilate toNORMOcarbiaPaCO2 = 35-40mmHg) • Avoid Hypoxia (PaO2 < 60mmHg or sat 90%) – maintain airway and oxygenation ↓O2 = bad
BRAIN VOLUME OSMOTIC AGENTS • Mannitol - Effects occur within 20 minutes; does not cross intact blood-brain barrier; observe for rebound ICP; 0.25-1 gm/kg IV over 24h • Frusemide10-20mg IV q6 hours. PRN ICP > 20. • Hypertonic Saline - When refractory to mannitol – 3% saline infusion or bolus – if serum osmolarity greater than 320 – hold no more benefit EUVOLEMIA CORTICOSTEROIDS • Decreases cerebral edema in brain tumors • Reduce CSF production, stabilize blood-brain barrier and cell membranes -> overall improvement of neuronal function • Dexamethasone
CSF VOLUME Drain CSF • Ventriculostomy– Pliable catheter inserted into lateral ventricle on nondominant side • Can remove CSF intermittently or continuously • Removal of even small amount will dramatically decrease ICP • Shunts
DECREASING METABOLIC DEMAND TEMPERATURE CONTROL • Antipyretic medications, cooling blanket SEIZURE CONTROL • Phenytoin: 15-18 mg/kg; not to exceed 50 mg/min • Diazepam: 5-10 mg bolus at 2 mg/min • Barbiturates (Pentobarbital & thiopental) when not responsive to conventional therapy SEDATION • Paralyzingagents; CV monitoring; endotracheal intubation; mechanical ventilation; ICP monitoring; arterial pressure monitoring • Reduce sympathetic tone ENVIRONMENT • dark room – free from noise minimise stimulus.
SURGICAL MANAGEMENT DecompressiveCraniectomy • Considered for IC-HTN refractory to medical treatment. Surgical Mx of subdural, epidural or intraparenchymal hematoma.