Download
1 / 45
450 likes | 695 Vues
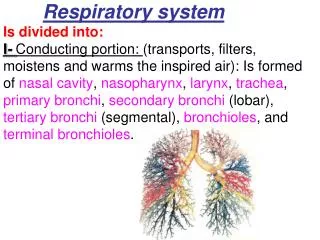
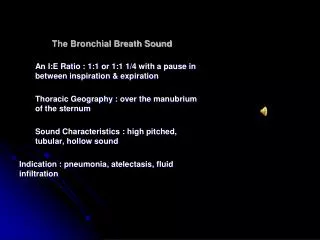
The Bronchial Breath Sound. An I:E Ratio : 1:1 or 1:1 1/4 with a pause in between inspiration & expiration Thoracic Geography : over the manubrium of the sternum Sound Characteristics : high pitched, tubular, hollow sound Indication : pneumonia, atelectasis , fluid infiltration.

E N D
The Bronchial Breath Sound An I:E Ratio : 1:1 or 1:1 1/4 with a pause in between inspiration & expiration Thoracic Geography : over the manubrium of the sternum Sound Characteristics : high pitched, tubular, hollow sound Indication : pneumonia, atelectasis, fluid infiltration
Vesicular Breath Sound An I:E Ratio : 1:0 or 1:1/4 with no pause in between inspiration & expiration Thoracic Geography : everywhere on the thoracic wall Sound Characteristics : low pitched, soft rustling sound Indication : pneumonia, atelectasis, fluid infiltration
Bronchovesicular Breath Sound An I:E Ratio : 1:1 or 1:1 1/4 with a pause in between inspiration & expiration Thoracic Geography : sternocostal margins, over the verbral column between the scapulae Sound Characteristics : high pitched, tubular, hollow sound Indication : pneumonia, atelectasis, fluid infiltration
Rales or crackles discontinuous sound Fine rales sound that you hear when burning wood crackles When fluid or mucus collects in the peripheral portions of the lung, the alveoli collapse and the walls of the alveoli stick together This is a sound heard during inspiration course rales
Pleural Friction Rubs Created when the visceral and parietal pleurae become inflammed and roughened The sound that a pleural friction rub makes is a leather-on-leather type of sound These sounds can be heard at the same points in the inhalatory and the exhalatory cycles
Bronchovesicular Breath Sound An I:E Ratio : 1:1 or 1:1 1/4 with a pause in between inspiration & expiration Thoracic Geography : sternocostal margins, over the verbral column between the scapulae Sound Characteristics : high pitched, tubular, hollow sound Indication : pneumonia, atelectasis, fluid infiltration
Rales or crackles discontinuous sound Fine rales sound that you hear when burning wood crackles When fluid or mucus collects in the peripheral portions of the lung, the alveoli collapse and the walls of the alveoli stick together This is a sound heard during inspiration course rales
Pleural Friction Rubs Created when the visceral and parietal pleurae become inflammed and roughened The sound that a pleural friction rub makes is a leather-on-leather type of sound These sounds can be heard at the same points in the inhalatory and the exhalatory cycles
Stridor High pitched wheezing that is caused by the obstruction of the trachea either by inflammation or an object Just enough air passes the obstructed point to cause a high-pitched whining wheeze In children, stridor is most frequently caused by croupe, a viral infection that causes the tracheal membranes to swell to a near-closed position The wheeze is produced much like a wind instrument produces sound through a wooden reed
Rhonchi or Wheezes The wheezes are considered to be central airway sounds caused by air passing through mucus plugs in the upper divisions of the tracheobronchial tree.
Stridor: Harsh, high-pitched, musical sound produced by turbulent airflow through partially obstructed upper airway • Supraglottic obstruction: Inspiratorystridor (high-pitched) • Extrathoracic trachea obstruction – includes glottis & subglottis: Biphasic stridor (intermediate pitch) • Intrathoracic trachea obstruction: Expiratory stridor (wheeze)
Chest &Lung • Respiratory Rhythm(Asthma,..) • Palpation • Crepitation in subcutaneous emphysema • Local tenderness , Axillary lymph node • Percussion • Hyperresonance or redused cardiac dullness • in emphysema or pneumothorax • Decreased resonance in consolidation
Chest &Lung • breathing sound: • Reduced:bronchiolitis,emphysema, pneumothorax, pleural effusion • Increased:consolidation,collapse • Bronchial:consolidation,collapse • Ronchi:bronchospasm,infection • Crepitation: infection • Wheezing:asthma • Vocal resonance:
Physiology of Murmurs • first and second sounds, or S1 and S2, which demarcate systole from diastole • S1 is the sound which marks the approximate beginning of systole, and is created when the increase in intraventricular pressure during contraction exceeds the pressure within the atria, causing a sudden closing of the tricuspid and mitral, or AV valves.
S2 • At the end of systole, the ventricles begin to relax, the pressures within the heart become less than that in the aorta and pulmonary artery, and a brief back flow of blood causes the semilunar valves to snap shut, producing S2. • Because diastole takes about twice as long as systole, there is a longer pause between S2 and S1 than there is between S1 and S2
During S1, the closing of the mitral valve slightly precedes the closing of the tricuspid valve, while in S2, the aortic valve closes just before the pulmonary valve. • the pressure during systole in the left ventricle is much greater than in the right, SO the mitral valve closes before the tricuspid in S1. • The pressure at the start of diastole in the aorta is much higher than in the pulmonary artery, the aortic valve closes first in S2.
The intensity of the murmur is next, graded according to the Levine scale: • I - Lowest intensity, difficult to hear even by expert listeners • II- Low intensity, but usually audible by all listeners • III - Medium intensity, easy to hear even by inexperienced listeners, but without a palpable thrill • IV - Medium intensity with a palpable thrill • V - Loud intensity with a palpable thrill. Audible even with the stethoscope placed on the chest with the edge of the diaphragm • VI - Loudest intensity with a palpable thrill. Audible even with the stethoscope raised above the chest.
Some times it is difficult to discern which is S1 and which is S2 ,So it is important to always palpate the PMI or the carotid or radial pulse when auscultating. The heart sound you hear when you first feel the pulse is S1, and when the pulse disappears is S2.
systole or diastole • where it is heard best • where it radiates to • if the murmur completely fills that phase of the cycle (i.e., holosystolic) • The quality and shape of the murmur(rumbling, blowing, machinery, scratchy, harsh, or musical) The intensity of the murmur(Levine scale) • if this murmur is clinically significant or not(physiologic flow murmurs :Pregnancy, Anemia,thyrotoxicosis,Innocent murmur )
physiologic murmurs • located between the apex and left lower sternal border • have minimal radiation • occur during early to mid-systole • have a crescendo-decrescendo shape, and a vibratory quality • usually change intensity with positional maneuvers, becoming quieter on standing and louder with squatting • A Valsalva maneuver will decrease the intensity of the murmur because the increase in intrathoracic pressure will decrease venous return, which will decrease flow through the heart and lessen the turbulence. • Additionally, they will not be correlated with additional audiologic findings, such as an S3 or S4.
Heart sound • Normal heart sound
aortic stenosis • systolic murmurs,heard best over the “aortic area” or right second intercostal space, with radiation into the right neck • harsh quality and may be associated with a palpably slow rise of the carotid upstroke • Symptoms: Angina, Syncope, Congestive heart failure • Early aortic stenosis • Late aortic stenosis
Mitral Regurgitation best heard at the apex, with radiation into the axilla holosystolic murmur congenital condition rheumatic heart disease marked left ventricular dilatation acute infective endocarditis acute or prior myocardial infarction
congenital disorders, such as tetralogy of Fallot, heard best in the pulmonic area, the second intercostal space on left sternal border radiating into the neck or the back has a crescendo-decrescendo shape, and a harsh quality Because it takes longer for the right ventricle to eject its load of blood through the stenotic valve, the closure of the pulmonary valve is delayed maneuvers which increase venous filling and blood flow into the right ventricle, such as deep inspiration, will tend to increase the intensity of the murmur. Pulmonary Stenosis
Aortic Regurgitation • Diastolic Murmurs • rheumatic heart disease, congenital ,endocarditis • blowing, decrescendo, and heard best in the third left intercostal space • In severe regurgitation, it may be holodiastolic • It radiates widely along the left sternal border
Mitral Stenosis • Diastolic Murmurs • best heard at the apex with little radiation • low-pitched, decrescendo, and rumbling • heard best with the patient in the left lateral decubitus position
Cardiovascular System • Inspection: Dyspnea,cyanosis,tachypnea,Edema, Clubbing,Apex beat,JVP,.. • Palpation: Thrill, Apex beat (Point of maximal impulse), All Pulses (arrrhythmia , weak or bounding pulse,absent femoral pulse) • Percussion: Diminished dullness(Pneumothorax ,Emphysema) • Auscultation: Heart rate • Newborn=70-120 Preschool child =75-120 • Infant=80-160 school child = 70-110
Cardiovascular System • Auscultation: Normal sinus dysrhythmia Rhythm(sinus arrhythmia,gallop rhythm, Heart sound(splitting S2,Ejection click ) Murmur site Intensity: grade 0-6 Timing:systolic(pan,early,late) or diastolic(early,mid,presystolic) Propagation:leftaxilla,neck,… Variation with position
Cyanosis and clubbing Cyanosis of the lips Pectus Carinatum pectus excavatum deformity
Breast • Breast of newborns are often enlarged due to maternal estrogen • Breast development 8-13 y/o • Breast development before 8 y/o are abnormal • Menarche occurs in breast stage 3 or 4 • In 10% of girls breasts develop asymmetry