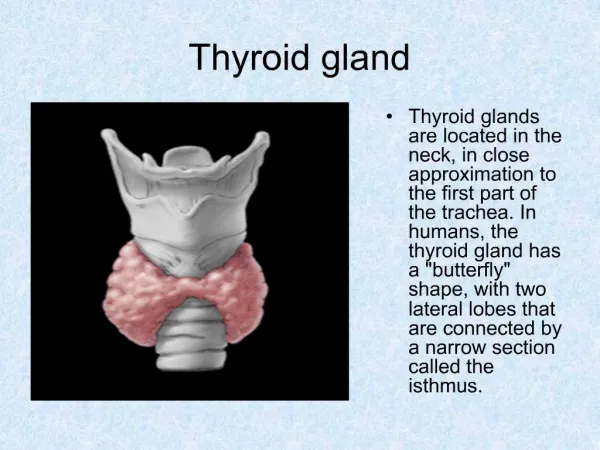
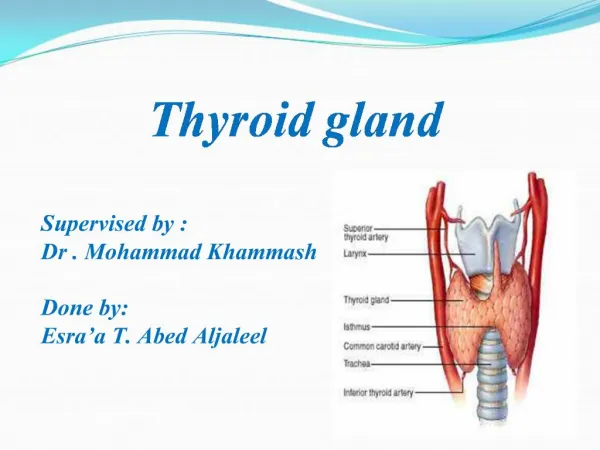
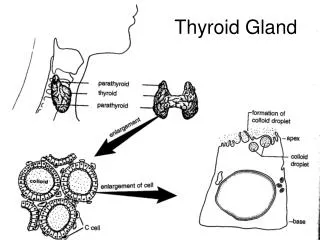
THYROID GLAND
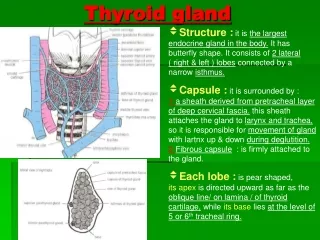
THYROID GLAND. Begashaw M (MD). Anatomy. Goiter. Generalized enlargement of the thyroid gland which is normally impalpable. Classification . 1. Simple- Euthyroid _Diffuse hyper plastic _( Multinodular ) 2. Toxic _Diffuse - Grave’s disease _Nodular


THYROID GLAND
E N D
Presentation Transcript
THYROID GLAND Begashaw M (MD)
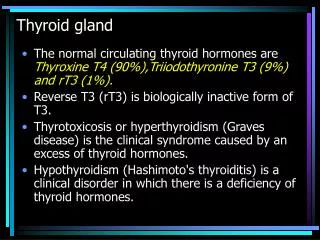
Goiter • Generalized enlargement of the thyroid gland which is normally impalpable
Classification 1. Simple-Euthyroid _Diffuse hyper plastic _(Multinodular) 2. Toxic _Diffuse - Grave’s disease _Nodular _Toxic adenoma 3. Neoplastic _ Benign _Malignant 4. Inflammatory _Autoimmune _Infectious _Acute –bacterial/viral _Chronic -tuberculous
Simple Goiter • Patho - physiology • enlargement of the thyroid gland • stimulation of the thyroid gland by high levels of circulating TSH • common in Females
Etiology _Iodine deficiency _Goitrogenscabagge _Drugs iodine,lithium _Defective hormone synthesis _peripheral resistance to thyroid hormone
Diffuse hyper-plastic goiter Persistent stimulation by TSH causes diffuse hyperplasia of the thyroid gland Soft, diffuse & large Usually occurs at puberty , pregnancy Areas of active lobule & inactive lobules
Nodular goiter • Nodular goiter -solitary -multinodular • Nodule -colloid when filled with colloid -cellular • Secondary changes -cystic degeneration -hemorrhage -calcification
Diagnosis • Clinical presentation _Discrete swelling in one lobe -Solitaryisolated -Dominant noduleabnormality Elsewhere _smooth, firm _painless _moves with swallowing _ euthyroid
Investigation • TFT T3, T4, TSH • CXR/Thoracic inlet x-rayscalcification, tracheal deviation & compression • Thyroid antibody titers • FNACytology
Complications Compression stridor, dysphagia, pain, & hoarseness Secondary thyrotoxicosis Carcinoma malignant changes of the follicular type
Prevention Introduction of iodized salt Thyroxin of 0.1mg daily Nodular stage is irreversible
Indication of surgery • Cosmetic • Tracheal compression • When malignancy cannot be excluded • Options of surgery _Near total thyroidectomy _Subtotal thyroidectomy
Toxic goiters • Thyrotoxicosis- increased metabolic rate due to high level of circulating thyroid hormone • 8X more commonly seen in females than males
Clinical features • symptoms _Loss of weight in spite of good appetite _preference of cold _Palpitation _Tiredness _Emotional liability • signs _excitability _presence of goiter _hot & moist palms _exophthalmus in primary type _tachycardia with cardiac arrhythmia
Diffuse Toxic GoiterGraves Disease Is a diffuse vascular goiter appearing at the same time as symptoms of hyperthyroidism Occurs in younger women Frequently associated with eye signs Hypertrophy & hyperplasia are due to abnormal TS antibodies F > M = 7:1
Toxic nodular goiter A simple nodular goiter is present for a long time before hyperthyroidismsecondarythyrotoxicosis Seen in middle aged/elderly people Less frequently associated with eye signs Nodules are inactive Intermediate thyroid tissue is involved in hyper secretion
Toxic nodule Solitary hyperactive nodule which may be part of a generalized nodularityor a true toxic adenoma is autonomous not due to TS antibodies normal thyroid tissue surrounding the nodule is suppressed & inactive
Diagnosis • Clinical picture • T3,T4,TSH • Isotope scanning
Treatment Antithyroid drugs Surgery Radioiodine
Anti thyroid Drugs used to resume the patient to a euthyroid state maintain this for a prolonged period cannot cure a toxic nodule
Surgery Preoperatively, the patient must be prepared with antithyroid drugs so that the patient becomes euthyroid Subtotal thyroidectomy
Post-operative complications Hemorrhage Respiratory obstruction Recurrent laryngeal nerve paralysis Thyroid insufficiency Parathyroid insufficiency Thyrotoxic crisis (storm) Wound infection
Thyroid Tumour • BenignFollicularadenoma • Malignant • Primary - EpithelialFollicular,Papillary,Anaplastic - Para follicularMedullary - Lymphoid cellslymphoma • Secondary - Metastatic - Local infiltrations
Benign Tumours • Follicular adenomas -solitary nodules -distinction between a follicular carcinoma &adenoma can only be made by histological examination -Treatment Lobectomy
Malignant Tumors • Clinical feature -Thyroid swelling -Enlarged cervical lymph node -papillary carcinoma -Recurrent laryngeal nerve paralysis –locally advanced disease -Anaplastic-hard, irregular, infiltrating
Investigations TFTT3,T4,TSH FNA Antibody assay Radio isotope scanning
Treatment/Prognosis _Surgerytotalthyroidectomy _Prognosis Histological type, age, extra thyroid spread, & size of tumor _ Males > 40 yrs of age & Females >50 yrs have worse prognosis _Distant metastatic diseaseworse prognosis
Anaplastic Carcinoma Mainly in elderly woman Local infiltration Epreadby lymphatics &blood stream Extremely lethal tumors with death occurring in most cases within month Present in advanced stages with tracheal obstruction Radiotherapy