Download
1 / 41
490 likes | 1.01k Vues
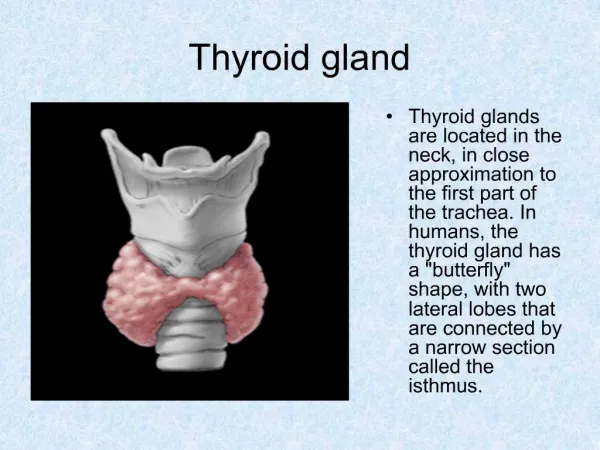
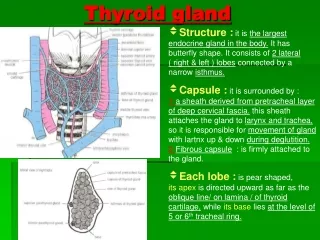
THYROID GLAND. MJ Noon 2014-57. Anatomy of the thyroid gland. • Light brown, firm organ • 15 – 20 gms in weight • Two lateral lobes connected by an isthmus • 4 x 2 cm in dimension; 20 – 40 mm thickness • Pyramidal lobe present in 80% of normal persons; usually left of midline

E N D
THYROID GLAND MJ Noon 2014-57
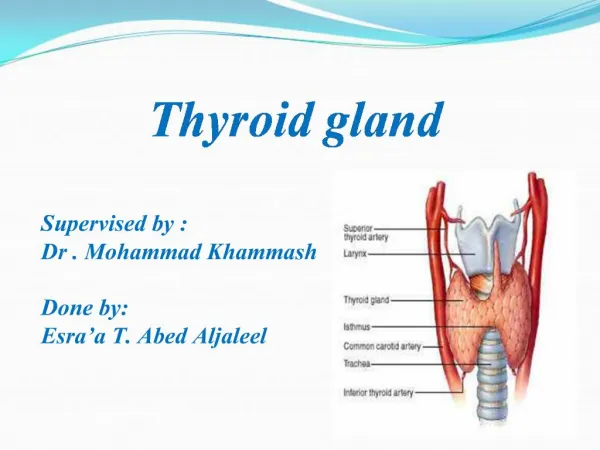
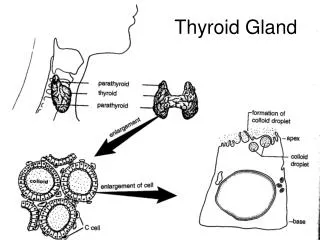
Anatomy of the thyroid gland •Light brown, firm organ •15 – 20 gms in weight •Two lateral lobes connected by an isthmus •4 x 2 cm in dimension; 20 – 40 mm thickness •Pyramidal lobe present in 80% of normal persons; usually left of midline •Four parathyroid glands closely related •Recurrent laryngeal nerves on both sides
Biosynthesis of T4 and T3 The process includes • Dietary iodine (I) ingestion • Active transport and uptake of iodide (I-) by thyroid gland • Oxidation of I- andiodination of thyroglobulin (Tg) tyrosine residues • Coupling of iodotyrosine residues (MIT and DIT) to form T4 and T3 • Proteolysis of Tg with release of T4 and T3 into the circulation
Normal circulatory concentrations • T4 4.5-11 g/dL • T3 60-180 ng/dL (~100-fold less than T4)
Carriers for Circulating Thyroid Hormones • More than 99% of circulating T4 and T3 is bound to plasma carrier proteins • Thyroxine-binding globulin (TBG), binds about 75% • Transthyretin (TTR), also called thyroxine-binding prealbumin (TBPA), binds about 10%-15% • Albumin binds about 7% • High-density lipoproteins (HDL), binds about 3% • Carrier proteins can be affected by physiologic changes, drugs, and disease
Thyroid Hormone Plays a Major Role in Growth and Development • Thyroid hormone initiates or sustains differentiation and growth • Stimulates formation of proteins • Is essential for normal brain development • Essential for childhood growth • Untreated congenital hypothyroidism or chronic hypothyroidism during childhood can result in incomplete development and mental retardation
Thyroid Hormones and the Central Nervous System (CNS) • Thyroid hormones are essential for neural development and maturation and function of the CNS • Decreased thyroid hormone concentrations may lead to alterations in cognitive function • Patients with hypothyroidism may develop impairment of attention, slowed motor function, and poor memory • Thyroid-replacement therapy may improve cognitive function when hypothyroidism is present
Thyroid Hormone Influences the Female Reproductive System • Normal thyroid hormone function is important for reproductive function • Hypothyroidism may be associated with menstrual disorders, infertility, risk of miscarriage, and other complications of pregnancy
Thyroid Hormone is Critical for Normal Bone Growth • T3 also may participate in osteoblast differentiation and proliferation, and chondrocyte maturation leading to bone ossification
Thyroid Hormone Regulates Mitochondrial Activity • T3 is considered the major regulator of mitochondrial activity • A potent T3-dependent transcription factor of the mitochondrial genome induces early stimulation of transcription and increases transcription factor (TFA) expression • T3 stimulates oxygen consumption by the mitochondria
Thyroid Hormones Stimulate Metabolic Activities in Most Tissues • Thyroid hormones (specifically T3) regulate rate of overall body metabolism • T3 increases basal metabolic rate • Calorigenic effects • T3 increases oxygen consumption by most peripheral tissues • Increases body heat production
Evaluation of patients with Thyroid gland disorder THREE MAIN CATEGORIES • HYPOFUNCTION • HYPERFUNCTION • ENLARGMENTS/GOITER • DIFFUSE ENLARGMENT • NODULAR ENLARGMENT
Clinical evaluation • HISTORY AND PHYSICAL EXAMINATION • Clinical manifestations: • HYPERFUNCTION • Weight loss, irritability, heat intolerance, thinning of hair, palpitations, tachycardia • HYPOFUNCTION • Weight gain, lethargy, coarse hair, cold intolerance, thick skin, slowed muscle reflex, constipation, slow mentation • GOITER • Anterior neck mass that moves on deglutition is thyroid gland in origin unless proven otherwise; enlarged thyroid gland • Physical Examination: • Accurate description of the thyroid gland and mass • Appreciate presence or absence of associated cervical lymphadenopathy
Thyroid Function Tests • T3 AND T4 LEVELS • Serum TSH and TRH • Free and bound ratio • Plain films; X-Rays(chest/thoracic inlet;clinical evidence of tracheal deviation,compression,retrosternal extension) • Ultrasonography(solid/cystic)or radioisotope scanning(99mTc-sodium pertechnate) for differentiating between • HOT nodules (actively functioning) • COLD nodules (non-functioning) • COOL (normaly functioning) • MRI and CT (EXTENT OF GOITRE) • FNAC(nature of thyroid nodules) • Thyroid antibodies
HYPERTHYROIDISM • Clinical syndrome of excess thyroid hormone in the circulation • Two dominant types or causes: • Grave’s disease • Toxic multinodular or solitary nodular goiter (Plummer’s disease) • Can be PRIMARY (increased Thyroid hormone independent of TSH) or SECONDARY (increased in hormone due to increased TSH)
HYPERTHYROIDISM/THYROTOXICOSIS • SIGNS • sinus Tachycardia • Hot,moist palms • Exosphthalmos • Lid lag • Agitation • Thyroid goitre • SYMPTOMS • Tiredness • Emotional lability • Heat intolerance • Wt.loss • Excessive appetite • palpitations
Graves’ disease (diffuse toxic goiter) • Most common cause of primary hyperthyrodism • Female dominant autoimmune disease • Inciting events; infection, steroid withdrawal, postpartum, iodide excess • Anti-TSH receptor antibodies(IgG),type2 hypersensitivity • TSI can cross placenta so neonatal thyrotoxicosis can occur • LABS; • Raised T3,T4 • Low TSH • TSH producing response to TRH is absent because of atrophy of pituitary TSH producing cells
Graves’ Disease • CLINACAL FEATURES; • INFILTRATIVE OPHTHALMOPATHY • Proptosis of eye(volume of retro-orbital connective tissue is increased; inflamation,GAGS,fattyinfiltration;orbital fibroblasts have TSH receptor and become targets of antibody attack) • Pretibialmyxedema( GAGS in dermis) • Thyroid acropachy; • Digital swelling • Finger clubbing • Cardiac problems;CHF,AF • Apathy,muscle weakness • thyromegaly
Graves’ Disease • Manage graves by 1)anti-thyroid drugs and,2)radioactive iodine ablation<CI in preg.> 3)surgery; subtotal-thyroidectomy
Multinodular Toxic Goiter (Plummer’s disease) • One or more thyroid nodules trapping and organifying more iodine and increase secretion of hormone independent of TSH control; autonomously functioning nodule/s • No exophthalmos or pretibialmyxoedema (Milder with no extrathyroidal manifestations) • Demonstrate increased uptake or radioactive iodine I131 localized to the nodule/s • Hot nodules on scan • Poor response to radioactive iodine treatment; surgery is the choice of management
Thyroid Storm • Rare but life-threatening complication of hyperthyroidism • Induced by thyroidal or non-thyroidal surgery; can be induced by infection or other forms of stress (eg. Labor & delivery, pulmonary infection, after RAI treatment) • Signs and symptoms of severe thyrotoxicosis • Hyperpyrexia, severe tachycardia, irritability, vomiting, diarrhea, and proximal muscle weakness; cause of death due to high cardiac output • Management: • Prevention is the best management • Immediate control of tachycardia, mechanical cooling, oxygen and volume resuscitation • Steroids • Intravenous beta-blockers (propranolol) • Anti-thyroid drugs and Iodine solution • Peritoneal dialysis in extreme cases
Hyperthyroidism DIFFUSE GLAND ENLARGMENT PRETIBIAL MYXEDEMA GRAVE’S OPHTHALMOPATHY
Hyperthyroidism DIAGNOSIS • History and Physical Examination • Thyroid Function tests • Radioactive iodine thyroid scan • Ultrasonography MANAGEMENT • MEDICAL MANAGEMENT • Anti-thyroid drugs (methimazole, PTU) • Beta-blockers (propranolol) • Radioactive Iodine • SURGERY • Subtotal thyroidectomy; Lobectomy • RADIOACTIVE IODINE TREATMENT • Diffuse = 7 – 9 mCi • Nodular = 12 – 15 mCi RADIOACTIVE IODINE SCAN (Iodine 131)
HYPOTHYROIDISM • Syndrome of deficient circulating levels of thyroid hormone • Cretinism in neonates – neurological impairment and mental retardation • Clinical manifestations: • Myxedema (severe form) • Bradycardia & cardiomegaly • Laboratory: • Decreased T3 and T4; Elevated TSH • Management: • Thyroxine replacement
THYROID CANCER • The most common endocrine malignancy that requires surgery • Included in the top 10 sites of malignancy for both sexes in the Philippines • Generally slow-growing and indolent malignancy • AGE – considered the most important prognostic factor • Certain types are also aggressive malignancy and potentially fatal disease
THYROID CANCER • MAJOR HISTOLOGIC TYPES • PAPILLARY THYROID CANCER • Most common (70%); well-differentiated • Slow-growing; lymphatic spread • Good prognosis • FOLLICULAR THYROID CANCER • Well-differentiated; 2nd most common (10%) • More aggressive; vascular invasion and spread • MIXED PAPILLARY-FOLLICULAR THYROID CANCER • Behaves and managed as papillary carcinoma • HURTHLE-CELL TUMOR • 5% incidence; intermediate differentiation • Behaves like follicular carcinoma but spread by lymphatics
THYROID CANCER • MAJOR HISTOLOGIC TYPES • LYMPHOMA (5%) • Usually in females; history of previous hashimoto’s • Surgery for compressive symptoms • Chemo and radiation sensitive • MEDULLARY THYROID CANCER • Aggressive; calcitonin producing tumor • 90% sporadic; 10% part of the MEN II syndrome • Does not uptake I131 • Poor prognosis; undifferentiated carcinoma • ANAPLASTIC THYROID CANCER • Worst prognosis; very aggressive • 30% developed from well-differentiated cancer (degeneration) • Chemo and radiation treatment • Palliatve surgery
THYROID CANCER • MANAGEMENT • SURGERY • LOBECTOMY + ISTHMUSECTOMY • TOTAL THYROIDECTOMY • INDICATED NECK DISSECTION • ADJUVANT TREATMENT • POSTOPERAIVE RADIOACTIVE IODINE TREATMENT • EXTERNAL BEAM RADIATION • CHEMOTHERAPY (emerging)
INDICATIONS FOR THE PERFORMANCE OF THYROID SURGERY • Thyroid enlargement (Goiter) causing compression symptoms (dysphagia, dyspnea) • Certain types of Hyperthyroidism • Thyroid Nodule/s or Thyroid Cancer • Cosmetic indication
Types of thyroid surgeries • SUBTOTAL-THYROIDECTOMY • TOTAL-THYROIDECTOMY(bilateral lobectomy) • ISTHMUSECTOMY • NEAR-TOTAL THYROIDECTOMY(total thyroid lobectomy on affected side with conservation of 1-2grm of thyroid on contralateral side to preserve blood flow to parathyroids
Complications of thyroid surgery • HAEMORRHAGE • NERVE DAMAGE • HYPOTHYROIDISM • HYPOPARATHYROIDISM • Wound infection(abscess must be drained) • Respiratory obstruction(kinking of trachea,laryngealoedema,trauma during intubation)