Chiari Malformation
Chiari Malformation. Presented by Abdulgadir F. Bugdadi. Types. Consists of 4 types. Probably unrelated to each other. Type 1 chiari malformation. Epidemiology. Age of presentation ( 12 – 73 ) average age is 40 years. Adults Slight female preponderance. Feature.

Chiari Malformation
E N D
Presentation Transcript
Chiari Malformation Presented by Abdulgadir F. Bugdadi
Types • Consists of 4 types. Probably unrelated to each other.
Epidemiology • Age of presentation ( 12 – 73) average age is 40 years. Adults • Slight female preponderance.
Feature • Heterogeneous entity but the common feature is ; Impaired CSF Circulation through Foramen magnum.
Components • Caudal displacement of Cerebellum with tonsillar herniation below foramen magnum. ( > 5mm below the foramen magnum , not essential and nor diagnostic). • Syringomyelia (30%-70%)…. • Hydrocephalus (7% - 9% in patients with 1&2)
Etiology • Different etiologies can be with it; • Small posterior fossa …. • Intracranial space occupying lesions .. • Lumboperitoneal shunt or multiple LP. “acquired, usually asymptomatic”. • Arachnoid web or scar or fibrosis around brainstem and tonsils around FM.
5. Abnormalities of upper cervical spines …. 6. Ehlers - Danlos syndrome. 7. Craniosynostosis.
Symptoms Asymptomatic 15% – 30%.
Signs Ataxia, corticospinal and sensory deficits, cerebellar signs and lower cranial nerve palsies. Loss of pain and temperature sensation, segmental weakness, syringomyelic syndrome or lower cranial nerve palsies ‘11%’. Ataxia, nystagmus (downbeat), dysarthria. Normal neurologic exam 10%
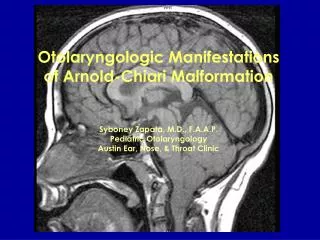
Imaging • MRI ; Diagnostic test of choice. Abnormalities that can be seen : • Tonsillar herniation. • Hydrosyringomyelia(20% - 30%). • Ventral brain stem compression. • Other findings ; Hydrocephalus or empty sella.
Cont. Other imaging • Cine MRI “CSF flow study”… • Myelography… • CT…
Treatment • Surgical management. • Goal of surgery ; Decompress the brain stem an reestablish normal CSF flow at the craniocervical junction. • Indication of surgery ; - Symptomatic. - Best response… - symptomatic & stable for years…
Surgery performed ; • Posterior fossa decompression (suboccipital craniectomy) +/- • Dural patch grafting. • Laminectomy of C1 (sometimes C2 or C3).
Feature • Caudally displaced cervicomedullary junction, pons, 4th ventricle and medulla. • Cerebellar tonsils located at or below foramen magnum. Usually associated with myelomeningocele and often accompanied by hydrocephalus.
Theory of pathophysiology • Primary dysgenesisof the brainstem with multiple other developmental anomalies. Not the result of tethering by the associated myelomeningocele.
Imaging • MRI ; • Primary findings: • “Z” bend deformity of medulla. • Cerebellar peg. • Tectal fusion “Tectalbeaking”. • Interthalamic adhesions. • Elongation/cervicalization of medulla. • Low attachement of tentorium.
B. Associated findings ; • Hydrocephalus. • Syringomyelia at cervicomedullary junction. • Trapped 4th ventricle. • Cerebellomedullary compression. • Agenesis/dysgenesis of corpus callosum.
Treatment • Insert CSF shunt for hydrocephalus (or check functioning of an existing shunt). • Surgical decompression is recommended for : (Argument) • Neurogenic dysphagia. • Neurogenic stridor. • Apneic spells. Note: Before recommending decompression always make sure that the patient has a functioning shunt.
Chiari type 3; 1. displacement of posterior fossa structures with cerebellum herniated through foramen magnum into cervical canal + high cervical or suboccipital encephalomeningocele. 2. Usually incompatible with life. • Chiari type 4; Cerebellar hypoplasia without cerebellar herniation.
END • Reference