The Respiratory System
The Respiratory System. Thorax and Lungs Rachel S. Natividad, RN, MSN, NP. Lobes and Landmarks. Performing the Assessment: Subjective Data. ROS -Ask about dyspnea, cough, chest pain (PQRST format) Short interview sessions if resp. distress / tiring easily. Inspection… …Always first!!!

The Respiratory System
E N D
Presentation Transcript
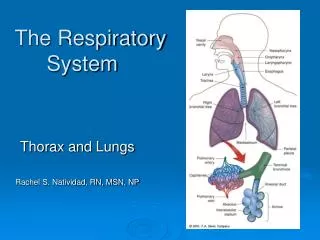
The Respiratory System Thorax and Lungs Rachel S. Natividad, RN, MSN, NP
Performing the Assessment: Subjective Data • ROS -Ask about dyspnea, cough, chest pain (PQRST format) • Short interview sessions if resp. distress / tiring easily
Inspection… …Always first!!! The moment you see the patient. What position is most comfortable for him? Does he appear relaxed, anxious, uncomfortable? Is he having any trouble breathing? Assessment begins…. Tripod Position
Focused Assessment • Inspection-cont. • Color, Size and shape & symmetry of chest, any lesions or scars • Anterior Lateral Posterior
Increased Anteroposterior:Transverse Diameter Altered size/shape:Barrel Chest 1:2 1:1
Fractured ribs/ flail chest Pneumothorax atelectasis paralysis of the diaphragm Spinal deformity Asymmetrical chest Scoliosis
Intercostal Spaces and Muscles Retractions
Focused Assessment Cont… • Resp. rate (per min.) and depth (shallow, even, deep) • Normal pattern of respiration – regular rhythm
Relating to other systems… • Skin: cyanosis, pallor • Nails: Clubbing • Spongy nail matrix and nail angle of greater than 160 degrees
Check for tenderness (normally nontender) Crepitus – SQ air pockets Tactile fremitus – increased with fluid accumulation Abnormal if tumor, fractured ribs, chest tubes, wound site, fluid Focused Assessment Cont.:Palpation
Continuous sounds Wheezes Sibilant Sonorous (Rhonchi) Discontinuous sounds Crackles (Rales) Fine Course *Atelectic crackles Stridor Pleural friction rub Adventitious/AbnormalBreath Sounds (T 11-2) p.132
Wheezes (Continuous) Sibililant wheeze Heard 1st in expiration • high-pitched musical sounds • Partial blockage in airflow Sonorous wheeze (rhonchi) Heard primarily in expiration • low pitched – snoring, rattling sound • Air passes through large airways filled with fluid/ secretions
Interpreting what you hear… • Is the sound is continuous or discontinuous? • Is the sound occur during inhalation or exhalation, or both?
Crackles (Discontinuous) • FINE vs. COURSE • Caused by collapsed or fluid-filled alveoli popping open • usually heard in the lung bases during inhalation • Atelectic crackles • Sridor • Pleural friction rub – pericarditis
Abnormal Breath Sounds • Diminished breathsounds • Absent breath sounds
Assessment Guide: Gas Exchange • Respiratory • Rate: 18 resp/min • Depth: deep, even, shallow • Effort: labored, unlabored • Breath Sounds • Describe: clear, rhonchi, inspiratory/expiratory wheezes, crackles • Location: all lobes, throughout lung fields, LLL, RUL/RML, lower lobes bilat. • Cough: present/not present • Describe: productive, moist, nonproductive • Sputum: large amount, thick yellow; moderate pink frothy sputum, sml. Amt. thin clear sputum.
Interventions in use: • Position, Turn, Cough, Deep breathe • O2 Method: nc, venti mask, rebreathing mask • Flow rate: 2L/min; 3l/min • Humidity: yes/no • Pulse Oximeter: continuous, spot monitoring • Incentive Spirometer: in use, n/a • Time used: 10 am, 11 am, 1 pm, 3 pm • Volume: 500 cc, 500 cc, 600 cc, 800 cc • Oropharyngeal Suctioning: Describe- moderate amount thick tan secretions • Med List: Albuterol inhaler, Prednisone, Theophylline