Enhancing Healthcare in Arunachal Pradesh: Improving Services and Infrastructure
260 likes | 419 Vues
Explore the best practices and initiatives in healthcare facilities in Arunachal Pradesh, focusing on key areas such as infrastructure, services provided, staff training, and quality assurance. Discover the challenges faced and the action taken to address them, ultimately aiming to enhance healthcare delivery in the region.

Enhancing Healthcare in Arunachal Pradesh: Improving Services and Infrastructure
E N D
Presentation Transcript
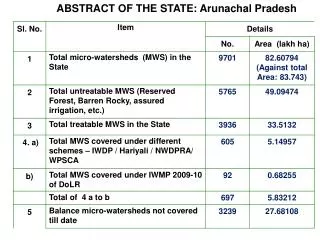
Positives • Overall Neat and clean infrastructure. Facilities have boundary walls, at places beautiful bamboo fencing and herbal garden • Dialysis unit: Machine, trained HR and Infrastructure available. • Basic ANC services provided. Early initiation of breast feeding practiced. • C-section available at General Hospital, East Siang and FRU, Ruksin. • Well functioning SNCU • State insurance with coverage up to Rs 2 lakhs for all patients.
Positives contd……. • ASHA : minimal attrition . Almost all ASHAs have bank account. • ANM and GNM school at GH and plans for starting BSc Nursing. • State Quality Assurance structures in place. • Funds being transferred online. HPDs given funds as per norms • Widespread Dengue outbreak in 2015 controlled well: one mortality. • Both the districts have dedicated TB hospitals
Major Findings • HR systems non existent: • Highly irrational posting especially in Sub centres • Ad-hoc recruitment, no skill assessment • Urban Health Centers – a place to accommodate personnel in HQ • Weak supportive supervision • Sub optimal service utilization: assured services not provided in facility and community despite adequate staffing.
Major Findings • Actual requirements of field not reflected in the plans and implementation: • No Micro-plans for VHND and due list for immunization • RNTCP Microscopy centers are under-utilized and cases sent directly to DH • Sub optimal utilization of NCD clinics at DH and CHC • Non Functioning MMU • No Condoms, OCPs, ECPs, Nischay kit in facilities except DH
Major Findings • High Out of pocket expenditure due to non availability of free drugs, diagnostics, dialysis initiatives and weak referral transport system • Districts unclear about Quality Assurance Program, still following ISO • Grievance redressal mechanism not found in any facility • Labour room protocols, partographs not practiced. Labour room nurses rotated every week • ASHA recruited last year, have not got any orientation training. Overall weak training system
Highly irrational posting especially in Sub centres Timeline March 2018 • Transfer order issued vide order No MEST-2016/88 dated Nlg the 13th May 2017 where 118 staffs transferred.(36 ANMs) link • East Siang -one facility namely SCTakilalung where 5 ANM were posted during the visit of 10th CRM team. Now 3 ANMs were posted out on 21st Nov’2016 vide order no. M-5271/T/P/11-12. • HRMIS is being implemented.
Ad-hoc recruitment, no skill assessment Timeline December 2017 • Contractual recruitment done at State HQ & regular through Public Service Commission, • They undergo induction training at State • Undergo continuing training on MH, CH, FP and other program to enhance their skill. • Currently, contractual recruitment on hold. • All recruitment through Public Service Commission only for Doctors. • Other category recruitment through state department central recruitment board (Written, practical & viva) • Recurrent baseline assessment ongoing for Nurses & LT and will scale up to include Doctors also
Urban Health Centers – a place to accommodate personnel in HQ • Current status of staff at UPHC following CRM:- At Pasighat 1 MO, 1 pharma, 2 GNM, 4 ANM, 1 LT, 2 FA, 1 Male Attendant, 1 N/Chowkidar, 1 Sweeper. At Naharlagun/Itanagar Transfer order issued vide order No MEST-2016/88 dated Nlg the 13th May 2017 (118 manpower transferred) Timeline December 2017
Weak supportive supervision • Difficult topography and poor road connectivity impedes on planned supportive supervision. • No proper monitoring vehicle in majority districts. Private vehicles used for Monitoring and supervision. • Supportive supervision plan in place at state • To place S/S plan at district • Technical support from DPs for NHPDs also Timeline December 2017
Sub optimal service utilization: assured services not provided in facility and community despite adequate staffing. • Functionality an issue due to irrational manpower placement • Basics services are provided in all functional SCs. • Beneficiaries prefer going to PHC/CHC/DH. • Functionalisation being initiated through rational posting • Regular review at district level planned • Regular S/S visit is being ensured from district & state • More training on all services ongoing and planned. Timeline September 2017
No Micro-plans for VHND and due list for immunization • Micro-plan for RI in place (Post MI) • 7 districts plan being corrected & improved. • Micro-plan and due list in place during MI rounds • Districts directed to generate due list for RI sessions also • Micro Plan for VHND available in 12 districts & rest furnishing shortly. Timeline September 2017
RNTCP Microscopy centers are under-utilized and cases sent directly to DH • Low population leading to low cases • Cases needing FNAC or complicated looking are referred to DH Timeline August 2017
Sub optimal utilization of NCD clinics at DH and CHC • It is a new programme • Systems to be placed and consolidated in all districts and functionalise clinics in health facilities. • Training ongoing at ToT level Timeline September 2017
Non Functioning MMU • 2 unit MMUs in 16 districts • MMU camp is conducted 6 camps per month (Ave). • MMU specific manpower not in place • Team constituted from among manpower in health facilities • Notice for combining School health mobile teams • Districts with fully non-functional MMUs identified and issued notice. Timeline August 2017
No Condoms, OCPs, ECPs, Nischay kit in facilities except DH • The observation has been reviewed for all districts • FP commodities now in place at districts • Condoms, OCPs, ECPs, Nischay kit received on 28/12/2016 and issued to all the facilities and ASHAs. • Supply chain management need revamping through use of IT (DVDMS) • More training being planned on FP services. Timeline August 2017
High Out of pocket expenditure due to non availability of free drugs, diagnostics, dialysis initiatives and weak referral transport system • The state Govt provides free drugs in the health facilities • State Govt provides fund for procurement of drugs (Health Deptt & DC) • Plan for Free diagnostic services under NHM will be shared during NPCC • PM Dialysis program underway. Tender floated on 30th May 2017 and by August, it should be functional in atleast 3 GHs. • JSSK in operation but need dramatic improvement at facilities • Plan for orientation of MO incharges of all facilities. • Quarterly Review Meeting of districts on NHM Performance at State Chaired by Commissioner (Health & Family Welfare) • Awareness on JSSK, JSY and free referral transport through IEC media including 102 ERC (in Place at Naharlagun) Timeline Dec 2017
Districts unclear about Quality Assurance Program, still following ISO • GH Pasighat was ISO certified. • Quality Assurance cell being improved • More orientation on importance of quality assurance for health staff planned. • Training on Quality assurance to Mos being planned. • Training of assessors, peer planned • Overall, National quality certification of DH planned. Timeline December 2017
Grievance redressal mechanism not found in any facility • Grievanceredressal mechanism through online system 104 EoI already floated. • 104 toll free no for comprehensive grievance (Health information, ASHA and any grievance) • Redressal mechanism is being inbuilt in the call centre. • Effective GR cell will be functionalised on hospitals and then to health facilities Timeline September 2017
Labour room protocols, partographs not practiced. LR nurses rotated every week • Due to shortage of Nurses, roration is practiced. • LR protocols are in place • It is a challenge to ensure use of Partograph even in the hospitals • More Doctors / Nurses are trained in SBA / BeMOC which will improve use. • Several notice issued for permanent posting of nurses to Labour / SNCU / ANC clinic and after 10th CRM too. Timeline Sept 2017
ASHA recruited last year, have not got any orientation training. Overall weak training system • Induction training of newly recruited Rural ASHA and Urban ASHA has been completed. • Orientation training of all existing ASHA done. • ASHA trainings started from Jan’2017. Timeline August 2017