Thoracic Outlet Syndrome
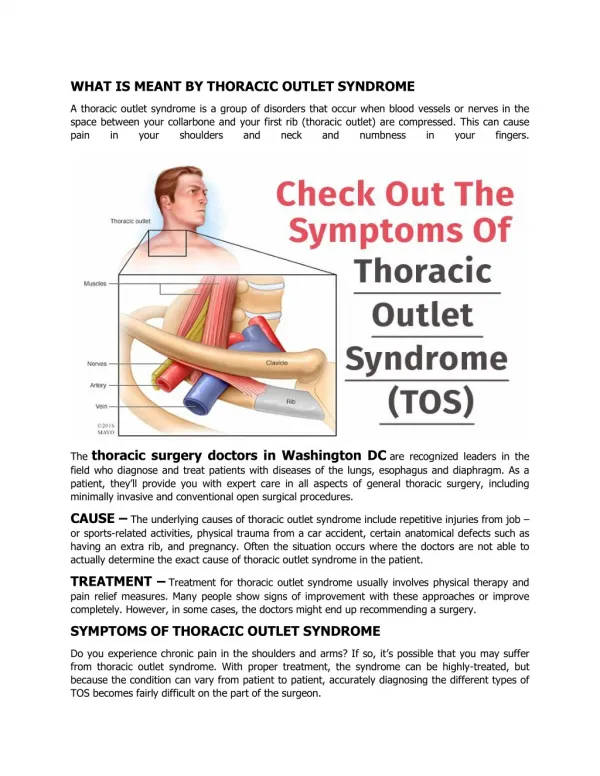
Thoracic Outlet Syndrome. It refers compression of subclavian vessels and brachial plexus at the superior aperture of the thorax. The symptoms can be neurologic or( and ) vascular. The pain may be atypical and predominant in the chest wall and parascapular area, simulating angina pectoris.

Thoracic Outlet Syndrome
E N D
Presentation Transcript
It refers compression of subclavian vessels and brachial plexus at the superior aperture of the thorax. • The symptoms can be neurologic or( and ) vascular. • The pain may be atypical and predominant in the chest wall and parascapular area, simulating angina pectoris.
4. Diagnosis of nerve compression can be determining the ulnar nerve conduction velocity( UNCV ). 5. Physiotherapy to improve posture, strengthen shoulder girdle, and stretch neck muscle is used initially. 6. Surgery includes extirpation the first rib, usually through transaxillary approach.
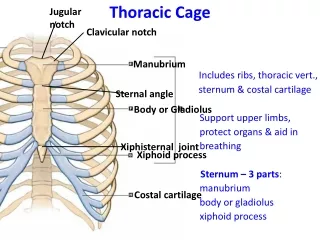
A. ANATOMIC CONSIDERATIONS A-0 • The subclavian vessels and brachial plexus transverse the cervicoaxillary canal into the arm. • The outer border of the first rib divides the canal into a proximal and a distal division. • The proximal division is composed of the scalene triangle and the space bounded by the clavicle and the first rib( costoclavicular space ).
A. ANATOMIC CONSIDERATIONS 4. The proximal division is the most critical for neurovascular compression. It is bounded superiorly by the clavicle and the subclavius muscle; inferiorly by the first rib; anteromedially by the sternum, clavipectal fascia and the costocoracoid ligament; and posterolaterally the scalenus media muscle and the long thoracic nerve.
A. ANATOMIC CONSIDERATIONS • The axilla, which is the outer division of the cervicoaxillary canal is bounded with pectoralis minor muscle, the coracoid process, and the head of humerus.
A-1 Compression Factors • Many factors can induce thoracic outlet syndrome, including congenital, trauma and atherosclerotic factors. 2. Bony abnormalities are present in 30% of patients, such as cervical rib, bifid first rib, fusion of first and second ribs or previous thoracoplasty.
A-2 Adson or Scalene Test 1. The patient is asked to (1) take and hold a deep breath (2) extend the neck fully (3) turn the face into one side. 2. It will tighten the anterior and middle scalene muscles. 3. Diminution or loss of the radial pulse suggests compression.
A-3 Costoclavicular Test( Military Position ) • The back is downward and backward. • The costoclavicular space will be narrowed by approximating the first rib and the clavicle. • Diminution or loss of the radial pulse suggests compression.
A-4 Hyperabduction Test 1. The arm is hyperabducted to 180 degrees. 2. Diminution or loss of the radial pulse suggests compression.
A-5 Arm Claudication Test • The shoulder is drawn backward and upward. The arm is raised horizontally with the elbow flexed 90 degrees. • With excise of hands, pain and numbness indicates compression.
B. SYMPTOMS AND SIGNS • Symptoms of never compression is present most frequently. • Pain and paresthesia are present in 95% of patients. • Motor weakness is present in 10% of patients. • Pain is insidious in onset and involves the neck, shoulder, arm or hand. • Atypical pain involving anterior chest wall and parascapular area is called pseudoangina.
B. SYMPTOMS AND SIGNS 5. Symptoms of vascular compression is less common than neurologic compression. 6. Symptoms of vascular compression includes coldness, weakness, fatigability of the hand and arm. Pain is more diffuse in distribution. 7. Raynaud’s phenomenon is occasionally seen.
B. SYMPTOMS AND SIGNS 8. Venous compression is recognized by venous distension, edema and discoloration of the hand and arm. 9. Thrombosis of the subclavian vein( “ effort thrombosis ” or Paget-Schroetter syndrome ) is infrequently.
B. SYMPTOMS AND SIGNS 10. However, objective physical findings are more in patients with vascular compression. 11. Objective physical findings of vascular compression are diminution or loss of the radial pulse in tests , Raynaud’s phenomenon, venous distension or edema… 12. Objective physical findings of neural compression are hypoesthesia, anesthesia and muscle weakness and atrophy.
C. DIAGNOSIS • PE, history, radiographs of chest and cervical spine, neuroloical consultation, EMG and UNCV. • Pulmonary, esophageal and chest wall causes must be ruled out.
C-1 Nerve Conduction Velocity • The normal average UNCV is 72m/sec across the thoracic outlet. • In patients of thoracic outlet syndrome, the average UNCV is 53m/sec( 32-65 m/sec ) across the thoracic outlet.
C-2 Angiography • Bruits in the supra- or infraclavicular spaces suggests stenosis, and absence of pulse denotes total occlusion. • Retro- or antegrade arteriograms of the subclavian and brachial arterial systems are indicated. • Phlebograph is indicated in patients of venous stenosis or obstruction.
C-3 Differentiated Diagnosis • Table 42-3
D. THERAPY • Physiotherapy is performed before surgery. • Physiotherapy includes heat massage, active neck exercise, scalenus anticus muscle stretching, strengthening of the upper trapezius muscle, and posture instrusion. • Most patients with a UNCV above 60 m/sec improve with phsiotherapy. • Most patients with a UNCV below 60 m/sec must undergo surgery with resection of the first rib and correction of other bony deformities.
D. THERAPY 5. Roos et al. suggested resection of the first rib, and a cervical rib when present, is best performed through the transaxillary approach, with decompression of 7th and 8th cervical and 1st thoracic root. 6. The anterior supraclavicular, infraclavicular and posterior approach were ever reported. 7. Posterior approach is especially important because 80% of patients are females.
D-1 Technique of Transaxillary Resection of First Rib • The patient was placed lateral position with involved arm abducted to 90 degrees. • A transaxillary incision was made between pectoralis major m. and latissimus dorsi m. • The insertion of the scalenus anticus m. on the first rib was dissected and muscle is divided. • The first rib is divided at middle portion. • The scalenus media m. can not be cut from the rib. The long thoracic nerve must be preserved.
D-1 Technique of Transaxillary Resection of First Rib 6. It is preferable to remove the entire first rib. 7. The periosteum should be fragmented and destoyed to avoid callus formation and “ regeneration “ of the rib. 8. Removal of incompletedly resected or regenerated rib and lysis of the brachial plexus can be done through posterior approach. 9. The anterior supraclavicular approach is used for arterial bypass and reconstruction.
D-2 Results • The results of first rib resection is good in 85%, fair in 10% and poor in 5%. • Uniform improvement of symptoms is usually in patients of primarily vascular compression. • There are 2 groups of patients, who have neural compression.
D-2 Results • The 1st group includes patients with ulnar neuralgia and diminution of radial pulse. 95% of this group are improved after first rib resection. • The 2nd group includes patients with atypical pain distribution with or without pulse change in compression tests. Although many patients can improve after first rib resection, the fair and poor results may mostly occur in the group.
D-2 Results 6. No hospital mortality is related directly to the procedure. 7. Morbidity includes pneumothorax, hematoma and infection.
E. PAGET-SCHROETTER SYNDROME • It refers “ effort “ thrombosis of the axillary-subclavian vein inducing by excessive or unusual use of the arm in addition to one or more compressive elements. • It is usually seen in professional athletes, Linotype operators, painters and beauticians. • Anticoagulants and conservative exercise can be used to treat it.
E. PAGET-SCHROETTER SYNDROME 4. First rib resection is indicated for patients with recurrent disease when returning to work. 5. Bypass with veins and other conduits has limited application.
F. RECURRENT THORACIC OUTLET SYNDROME • 10% of surgically treated patients have shoulder, arm or hands pain and pareathesia. Most patients can be relieved with physiotherapy and muscle relaxant. • In 1.6% of patients, symptoms exacerbate and persist. • Most recurrences occur in 3 months postoperatively.
F. RECURRENT THORACIC OUTLET SYNDROME 4. Pseudorecurrence (1) A 2nd rib was mistakenly resected for a 1st rib (2) A 1st rib was resected but a cerical rib was left. (3) A cervical rib was resected but an abnormal 1st rib was left. (4) A 2nd rib was resected but a rudimentary 1st rib was left.
F. REC F. RECURRENT THORACIC OUTLET SYNDROME 5. True recurrence The 1st rib was not resected completely. 6. All patients with recurrence after 1st rib resection should undergo physiotherapy. If symptoms persist and UNCV is still low then re-operation is indicated. 7. Re-operation is always done through the posterior thoracoplasty approach.
F. RECURRENT THORACIC OUTLET SYNDROME 8. The anterior or supraclavicular approach is not adequate for re-operation. 9. The basic elements for re-operation are (1) resection of recurrent or persistent bony remnants (2) neurolysis of the brachial plexus or nerve roots (3) dorsal sympathectomy of T1, T2, T3 ganglia
F. RECURRENT THORACIC OUTLET SYNDROME 10. The technique includes a high thora- coplasty incision, extending 3 cm above the angle of the scapula, halfway between the angle of the scapula and spinous processes, and caudate 5 cm from the angle of scapula. 11. The trapezius and rhomboid muscles are divided..
F. RECURRENT THORACIC OUTLET SYNDROME 12. The scapula is retracted by incision of the LD muscle over the 4th rib. • The posterior superior serratus muscle was divided and sacrospinalis muscle is retracted medially. 14. The 1st and cervical rib must be resected, if present subperiosteally. 15. The regenerated periosteum is extirpated.
F. RECURRENT THORACIC OUTLET SYNDROME 16. If excessive scar is present the it is necessary to perform sympathectomy initially. This involves resection of a 1- inch segment of 2nd rib posteriorly to locate the sympathetic ganglia. 17. Neurolysis is performed using a nerve stimulator but not into the sheath.
F. RECURRENT THORACIC OUTLET SYNDROME 18. A J-P drain is left in the area of brachial plexus. Depo-Medral, 80 mg, is left in the area of brachial plexus. 19. The arm is kept in sling to be used gently for 3 months. 20. When the problem is vascular, involving false or mycotic aneurysms, bypass graft is interposed. The saphenous vein is usually used.
F. RECURRENT THORACIC OUTLET SYNDROME 21. 7% of patients underwent 2nd re-operation for rescarring. No death occurred. Only one patient had infection and needed drainage.