Spinal Cord Injuries
1.21k likes | 1.7k Vues
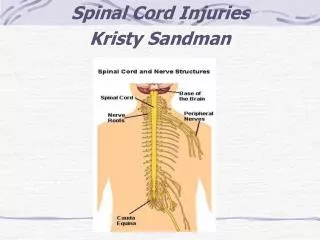
Spinal Cord Injuries. Dr Mohamed abdul jalil altamimi Consultant neurosurgeon Department of surgery 2016-2017. Basic Anatomy and Physiology. What is the anatomy of the spinal cord on cross section?.

Spinal Cord Injuries
E N D
Presentation Transcript
Spinal Cord Injuries Dr Mohamed abdul jalil altamimi Consultant neurosurgeon Department of surgery 2016-2017
What is the anatomy of the spinal cord on cross section? On cross section; ascending (conveying information to the brain) and descending (conveying information from the brain) tracts.
What is the anatomy of the spinal cord on cross section? On cross section; breathing and voiding.
From a surgeon’s perspective, the layers to get to the spinal cord.
From a surgeon’s perspective, the layers to get to the spinal cord.
What are the clinically important ascending tracts and where do they cross over? Explain Brown Sequard if somebody stabs you in the Right hemicord: pain is abolished in the left leg (pin prick), fine touch is abolished in the right leg (light touch).
What are the clinically important descending tracts and where do they cross over? Paralysis on the same side in Brown Sequard example (right leg)
At what level does the spinal cord end and why is it important? Can a cauda equina syndrome give you complete paralysis of the legs? Only if it is at L2!
What are the differences between UMN and LMN? (e.g., cauda equina vs. myelopathy)
Acute vs. chronic injuries;complete vs. incomplete injuries • “Acute”=sudden onset of symptoms • “Complete” ?
What is a complete spinal cord injury? • “Complete” = absence of sensory and motor function in the perianal area (S4-S5)
Terminology • Plegia = complete lesion • Paresis = some muscle strength is preserved • Tetraplegia (or quadriplegia) • Injury of the cervical spinal cord • Patient can usually still move his arms using the segments above the injury (e.g., in a C7 injury, the patient can still flex his forearms, using the C5 segment) • Paraplegia • Injury of the thoracic or lumbo-sacral cord, or cauda equina • Hemiplegia • Paralysis of one half of the body • Usually in brain injuries (e.g., stroke)
What are the important vegetative functions and when are they affected?
Reflexes • Deep Tendon Reflexes • Arm • Bicipital: C5 • Styloradial: C6 • Tricipital: C7 • Leg • Patellar: L3, some L4 • Achilles: S1 • Pathological reflexes • Babinski (UMN lesion) • Hoffman (UMN lesion at or above cervical spinal cord) • Clonus (plantar or patellar) (long standing UMN lesion)
What is and how do you determine the level of injury? • Motor level = the last level with at least 3/5 (against gravity) function • NB: this is the most important for clinical purposes • Sensory level = the last level with preserved sensation • Radiographic level = the level of fracture on plain XRays / CT scan / MRI • NB: spine level does not correspond to spinal cord level below the cervical region
Case scenario • 25 y/o white male • Fell off the roof (20 feet) • Had to be intubated at the scene by EMS • Consciousness regained shortly thereafter • Could not move arms or legs • Could close and open eyes to command • Not able to breathe by himself–totally dependent on mechanical ventilation
High cervical injuries (C3 and above) • Motor and sensory deficits involve the entire arms and legs • Dependent on mechanical ventilation for breathing (diaphragm is innervated by C3-C5 levels)
Case scenario • 19 y/o white male • Diving accident (shallow water) • No loss of consciousness • Could not understand why he could not move his legs, forearms and hands (he could shrug shoulders and elevate arms) • BP 75/40, HR 54/’ • Had difficulties breathing and required intubation a few hours after the accident
Midcervical injuries (C3-C5) • Varying degrees of diaphragm dysfunction • Usually need ventilatory assistance in the acute phase • Shock
What is the difference between spinal shock and neurogenic shock?
Neurogenic shock • Seen in cervical injuries • Due to interruption of the sympathetic input from hypothalamus to the cardiovascular centers • Hallmark: hypotension (due to vasodilation, due to loss of sympathetic tonic input) is associated with bradycardia (not tachycardia, the usual response), due to inability to convey the information to the vasomotor centers in the spinal cord
Low cervical injuries (C6-T1) • Usually able to breathe, although occasionally cord swelling can lead to temporary C3-C5 involvement (need mechanical ventilation) • The level can be determined by physical exam
So what do you expect with a cervical lesion? • Quadriplegia or quadriparesis • Bowel/bladder retention (spastic) • Various degrees of breathing difficulties • Neurogenic and/or spinal shock
Case scenario • 22 y/o female • Motor vehicle accident (hit a pole at 60mph) • Short term loss of consciousness (10’) • Not able to move or feel her legs • No bladder / bowel control or sensation • Sensory level at the umbilicus
Thoracic injuries (T2-L1) • Paraparesis or paraplegia • UMN (upper motor neuron) signs
Case scenario • 22 y/o female • Motor vehicle accident • Not able to move or feel her legs below the knee • Could flex thighs against gravity • No bladder / bowel control or sensation • Sensory level above the knee on L, below the knee on R
Cauda equina injuries (L2 or below) • Paraparesis or paraplegia • LMN (lower motor neuron) signs • Thigh flexion is almost always preserved to some degree
What is the difference between cauda equina and conus medullaris syndrome?
Anterior cord syndrome • Loss of motor, pain and temperature • Preserved propioception and deep touch
What is the central cord syndrome? • Cervical spinal cord involvement with arms more affected than legs • May occur with trauma, tumors, infections, etc • Traumatic lesions tend to improve in 1-2 weeks • Surgical decompression may be indicated if there is spinal stenosis
Goal of spine trauma care • Protect further injury during evaluation and management • Identify spine injury or document absence of spine injury • Optimize conditions for maximal neurologic recovery
Suspected Spinal Injury • High speed crash • Unconscious • Multiple injuries • Neurological deficit • Spinal pain/tenderness • Up to 15% of spinal injuries have a second (possibly non adjacent) fracture elsewhere in the spine
Initial Management • Immobilization • Rigid collar • Sandbags and straps • Spine board • Log-roll to turn • Prevent hypotension • Pressors: Dopamine, not Neosynephrine • Fluids to replace losses; do not overhydrate • Maintain oxygenation • O2 per nasal canula • If intubation is needed, do NOT move the neckAdvance Trauma Life Support (ATLS) guidelines
Management in the hospital • NGT to suction • Prevents aspiration • Decompresses the abdomen (paralytic ileus is common in the first days) • Foley • Urinary retention is common • Methylprednisolone (Solu-Medrol) • Only if started within 8 hours of injury • Exclusion criteria • Cauda equina syndrome • GSW • Pregnancy • Age <13 years • Patient on maintenance steroids
Radiolographic evaluation X-ray Guidelines (cervical) AABBCDS • Adequacy, Alignment • Bone abnormality, Base of skull • Cartilage • Disc space • Soft tissue
Adequacy • Must visualize entire C-spine • A film that does not show the upper border of T1 is inadequate • Caudal traction on the arms may help • If can not, get swimmer’s view or CT
Alignment • The anterior vertebral line, posterior vertebral line, and spinolaminar line should have a smooth curve with no steps or discontinuities • Malalignment of the posterior vertebral bodies is more significant than that anteriorly, which may be due to rotation • A step-off of >3.5mm is significant anywhere
Lateral Cervical Spine X-Ray • Anterior subluxation of one vertebra on another indicates facet dislocation • < 50% of the width of a vertebral body unilateral facet dislocation • > 50% bilateral facet dislocation
Disc Disc Spaces Should be uniform Assess spaces between the spinous processes
Soft tissue Nasopharyngeal space (C1) 10 mm (adult) Retropharyngeal space (C2-C4) 5-7 mm Retrotracheal space (C5-C7) 14 mm (children) 22 mm (adults)
AP C-spine Films Spinous processes should line up Disc space should be uniform Vertebral body height should be uniform. Check for oblique fractures.
Open mouth view Adequacy: all of the dens and lateral borders of C1 & C2 Alignment: lateral masses of C1 and C2 Bone: Inspect dens for lucent fracture lines