Arterial Blood Gas Interpretation Sam Ravenscroft
MedEd 2 MEDICAL STUDENT. Arterial Blood Gas Interpretation Sam Ravenscroft. What does an ABG tell us?. Provides a rapid assessment of the patient’s respiratory and biochemical physiology. Useful information from blood gas: Respiratory Physiology Acid Base Balance

Arterial Blood Gas Interpretation Sam Ravenscroft
E N D
Presentation Transcript
MedEd 2 MEDICAL STUDENT Arterial Blood Gas Interpretation Sam Ravenscroft
What does an ABG tell us? Provides a rapid assessment of the patient’s respiratory and biochemical physiology • Useful information from blood gas: • Respiratory Physiology • Acid Base Balance • Electrolytes • Extras • Glucose • Lactate
My system for interpreting the ABG 1. Clinical context 2. Respiratory failure? 3. Outline abnormal values 4. Acidosis or Alkalosis? 5. Respiratory or Metabolic? 5ii(if metabolic acidosis) Anion Gap 6. Compensated or uncompensated? 7. Why?
1. Clinical context Clinical picture can point you in the right direction before you even start: • History of anxiety ---> resp. alkalosis • History of diabetes ---> DKA? It can also alert you to “false normals”: • Normal PaCO2 in asthma attack • Normal PaO2 on high flow oxygen
2. Respiratory failure? On room air, PaO2 should be > 10kPa PaO2 < 10kPa is hypoxic PaO2 < 8kPa is respiratory failure Type 1 respiratory failure: PaO2 < 8kPa Type 2 respiratory failure: PaO2 < 8kPa and PaCO2 > 6kPa
3. Outline abnormal values This step is fairly self-explanatory....
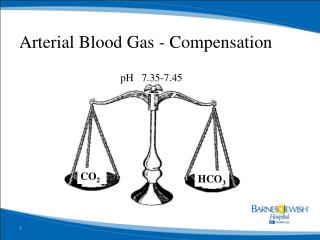
4. Acidosis or Alkalosis? Use the pH to decide this PaCO2 skewed in the oppositedirection to pH means the disturbance is respiratory PaCO2 skewed in the samedirection as pH OR an abnormal pH with a normal PaCO2 means the disturbance is metabolic 5. Respiratory or Metabolic? ROMERespiratory Opposite Metabolic Equal
5. Respiratory or Metabolic? RespiratoryAlkalosis Metabolic Alkalosis pH Metabolic acidosis RespiratoryAcidosis PaCO2
6. 6. Compensated or uncompensated? For respiratory disturbance: Metabolic compensation can occur by altering the bicarbonate (normal 22-28) For metabolic disturbance: Respiratory compensation can occur by regulating PaCO2
Example 1 • 60 year old woman on the orthopaedic ward, recent hip replacement, has become short of breath • pH: 7.48 • pO2: 8.0 kPa • pCO2: 3.2 • HCO3-: 24 mmol/l There is alkalaemia pH and pCO2 are changed in different directions -> respiratory alkalosis 1. Clinical context 2. Respiratory failure? 3. Outline abnormal values 4. Acidosis or Alkalosis? 5. Respiratory or Metabolic? 6. Compensated or uncompensated?
Example 2 • 20 year old man in A&E, feeling very unwell, thirsty and drinking lots of fluids • Na+: 148 mmol/l • K+: 3.5 mmol/l • Cl-: 100 mmol/l • pH: 7.32 • pO2: 11.5 • pCO2: 3.0 kPA • HCO3-: 18 mmol/l • Glucose : 30 mmol/l 1. Clinical context 2. Respiratory failure? 3. Outline abnormal values 4. Acidosis or Alkalosis? 5. Respiratory or Metabolic? 6. Compensated or uncompensated?
5a. Anion Gap (Na+ + K+) - (Cl- + HCO3-) Should be 15-20 • Causes of a raised anion gap: Excess anions! • Ketoacidosis (ETOH, diabetes, starvation) • Uraemia • Salicylates • Methanol • Aldehydes • Lactic acidosis • Ethylene glycol (Antifreeze)
Example 2 • 20 year old man in A&E, feeling very unwell, thirsty and drinking lots of fluids • Na+: 148 mmol/l • K+: 3.5 mmol/l • Cl-: 100 mmol/l • pH: 7.32 • pO2: 11.5 • pCO2: 3.0 kPA • HCO3-: 18 mmol/l • Glucose : 30 mmol/l There is acidaemia The pH and the pCO2 are both low -> metabolic acidosis AG = 148 - 100 - 18 = 30 KUSMALE
More examples! Split up into smaller groups to go through these with a tutor
Example 3 • 44 year old man in A&E (BG: Ulcerative Colitis) severe diarrhoea for 2 days • Creatinine: 200 umol/l • Urea: 17 • Na+: 135 mmol/l • K+: 3.1 mmol/l • Cl-: 113 mmol/l • pH: 7.31 • pO2: 12.5 • pCO2: 4.0 kPA • HCO3-: 14 mmol/l
Example 4 • 78 year old man hx of severe COPD, • pH: 7.34 • pO2: 9.0 kPA • pCO2: 7.9 • HCO3-: 32 mmol/l
Example 5.1 • 20 year old woman with severe asthma in A&E, very short of breath, speaking in single words, on 15l O2 • pH: 7.47 • pO2: 11.2 kPA • pCO2: 3.7 kPA • HCO3-: 25 mmol/l
Example 5.2 • 20 year old woman with severe asthma in A&E, • She is treated with back to back nebulisers, IV magnesium and IV aminophylline, but 30 minutes later she is not improved • pH: 7.32 • pO2: 8.8 kPA • pCO2: 6.2 kPA • HCO3-: 25 mmol/l
Example 6 • 30 year old man in A&E (BG: T1DM) has abdominal pain and vomiting • Na+: 134 mmol/l • K+: 5.8 mmol/l • Cl-: 96 mmol/l • pH: 7.32 • pO2: 12.1 kPA • pCO2: 3.2 kPA • HCO3-: 18 mmol/l
Example 7 • 66 year old man admitted with AKI ? cause • Albumin: 38 g/l (n=40 g/l) • Na+: 135 mmol/l • K+: 5 mmol/l • Cl-: 102 mmol/l • Urea: 8.2 mmol/l • Creatinine 115 umol/l • pH: 7.28 • pCO2: 4.7 kPA • HCO3-: 16 mmol/l • Lactate: 5.7