Arterial Blood Gas Interpretation
Arterial Blood Gas Interpretation. Dr. Kapila Hettiarachchi shaankh@icloud.com. Acid-base Balance Henderson- Hasselbalch Equation. [HCO 3 - ] pH = pK + log ---------------- .03 [PaCO 2 ]

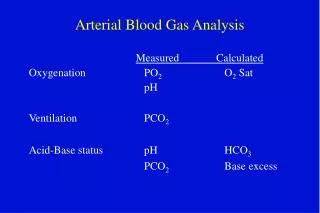
Arterial Blood Gas Interpretation
E N D
Presentation Transcript
Arterial Blood Gas Interpretation Dr. KapilaHettiarachchi shaankh@icloud.com
Acid-base Balance Henderson-Hasselbalch Equation [HCO3-] pH = pK + log ---------------- .03 [PaCO2] For teaching purposes, the H-H equation can be shortened to its basic relationships: HCO3- pH ~ --------- PaCO2
pH is inversely related to [H+]; a pH change of 1.00 represents a 10-fold change in [H+] pH [H+] in nanomoles/L 7.00 100 7.10 80 7.30 50 7.40 40 7.52 30 7.70 20 8.00 10
Acid-base Terminology • Primary acid-base disorder: One of the four acid-base disturbances that is manifested by an initial change in HCO3- or PaCO2. • Metabolic acidosis (MAc), Metabolic alkalosis (MAlk), • Respiratoryacidosis (RAc), and Respiratory alkalosis (RAlk). • Compensation: The change in HCO3- or PaCO2 that results from the primary event.
Respiratory Acid-base Disorders:Some Clinical Causes RESPIRATORY ALKALOSIS↓PaCO2 &↑pH Hypoxemia (includes altitude) Anxiety Sepsis Any acute pulmonary insult (e.g., pneumonia, mild asthma attack, early pulmonary edema, pulmonary embolism)
Primary Acid-base Disorders:Respiratory Alkalosis • Respiratory alkalosis Primary EventCompensatory Event HCO3-Reduced HCO3- HighpH ~ ---------- ---- High pH ~ ------------------- Low PaCO2 Low PaCO2
Expected changes in pH and HCO3- for a 10-mm Hg change in PaCO2 resulting from respiratory alkalosis: ACUTE CHRONIC pH ↑ by 0.08 pH ↑ by 0.04 HCO3-↓ by 2 HCO3-↓ by 5 * Units for HCO3- are mmol/L
Respiratory Acid-base Disorders:Some Clinical Causes RESPIRATORY ACIDOSIS↑PaCO2 & ↓pH Central nervous system depression (e.g., drug overdose) Chest bellows dysfunction (e.g., Guillain-Barré syndrome, myasthenia gravis) Disease of lungs and/or upper airway (e.g., chronic obstructive lung disease, severe asthma attack, severe pulmonary edema)
Primary Acid-base Disorders:Respiratory Acidosis • Respiratory acidosis – Primary Event Compensatory Event HCO3- Increased HCO3- Low pH ~ --------- Low pH ~ ------------------- High PaCO2 High PaCO2
Expected changes in pH and HCO3- for a 10-mm Hg change in PaCO2 resulting from respiratory acidosis ACUTE CHRONIC pH ↓ by 0.07 pH ↓ by 0.03 HCO3-↑ by 1* HCO3-↑ by 3 - 4 * Units for HCO3- are mmol/L
Metabolic Acid-base Disorders: Some Clinical Causes METABOLIC ALKALOSIS↑ HCO3- & ↑pH • Chloride responsive (responds to NaCl or KCl therapy): diuretics, corticosteroids, gastric suctioning, vomiting • Chloride resistant: any hyperaldosterone state (e.g., Cushing’s syndrome, Bartter’s syndrome, severe K+ depletion)
Primary Acid-base Disorders: Metabolic Alkalosis Metabolic alkalosis Primary Event Compensatory Event HighHCO3- High HCO3- High pH ~ --------------- High pH ~ -------------------- PaCO2Increased PaCO2
Metabolic Acid-base Disorders: Some Clinical Causes METABOLIC ACIDOSIS↓HCO3- & ↓pH - Increased anion gap • lactic acidosis; ketoacidosis; drug poisonings (e.g., aspirin, ethylene glycol, methanol) - Normal anion gap • diarrhea; some kidney problems (e.g., renal tubular acidosis, interstitial nephritis)
Primary Acid-base Disorders: Metabolic Acidosis Metabolic acidosis Primary Event Compensatory Event Low HCO3- Low HCO3- Low pH ~ ------------ Low pH ~ ------------ PaCO2 Decreased PaCO2
Metabolic Acidosis – How to detect compensation "Winter's formula":
Anion Gap Metabolic acidosis is conveniently divided into elevated and normal anion gap (AG) acidosis. AG is calculated as AG = Na+ - (Cl- + HCO3- ) Note: Normal AG is typically 12 ± 4 mEq/L.
Mixed Acid-base Disorders are Common • In chronically ill respiratory patients, mixed disorders are probably more common than single disorders, e.g., RAc + MAlk, RAc + Mac, Ralk + MAlk.
Met. Alkalosis + Met. Acidosis • In renal failure (and other conditions) combined MAlk + MAc is also encountered. • Always be on the lookout for mixed acid-base disorders. They can be missed!
For an increased anion gap metabolic acidosis, are there other derangements? • Determining the “corrected bicarbonate concentration”: Corrected HCO3 = measured HCO3 + (Anion Gap - 12) • If the corrected HCO3 is less than normal (under 22mEq/L) then there is an additional metabolic acidosis present. • Corrected HCO3 values over 26 mEq/L reflect a co-existing metabolic alkalosis. • If it remains between 22-26mEq/L only existing Met. Acidosis is present
Correction of severe acidosis Give NaHCO3 only If PH is < 7.1 but not in respiratory acidosis NaHCO3 in mmol = Base deficit X Body weight 3 Give half of that Target is keeping PH > 7.2 NaHCO3 1 mmol per Kg will be enough if ABG not available
Tips to Diagnose Mixed Acid-base Disorders TIP 1. Do not interpret any blood gas data for acid-base diagnosis without closely examining the serum electrolytes: Na+, K+, Cl-, and CO2. • A serum CO2 out of the normal range always represents some type of acid-base disorder • Note that serum CO2 may be normal in the presence of two or more acid-base disorders.
Tips to Diagnose Mixed Acid-base Disorders (cont.) TIP 2. Single acid-base disorders do not lead to normal blood pH. Although pH can end up in the normal range (7.35 - 7.45) with a single mild acid-base disorder, a truly normal pH with distinctly abnormal HCO3- and PaCO2 invariably suggests two or more primary disorders. .
Tips to Diagnose Mixed Acid-base Disorders (cont.) Example: pH 7.40, PaCO2 20 mm Hg, HCO3- 12 mEq/L in a patient with sepsis. Normal pH results from two co-existing and unstable acid-base disorders – acute respiratory alkalosis and metabolic acidosis .
Acid-base Disorders: Test Your Understanding A child with severe asthma, arterial blood gas shows pH of 7.14 PaCO2 of 70 mm Hg HCO3- of 23 mEq/L How would you describe the likely acid-base disorder(s)?
Acid-base Disorders: Test Your Understanding - Answers Acute elevation of PaCO2 leads to reduced pH, i.e., an acute respiratory acidosis. However, is the problem only acute respiratory acidosis or is there some additional process? For every 10-mm Hg rise in PaCO2 (before any renal compensation), pH falls about 0.07 units. Because this patient's pH is down 0.26, or 0.05 more than expected for a 30-mm Hg increase in PaCO2, there must be an additional metabolic problem. Also note that with acute CO2 retention of this degree, the HCO3- should be elevated 3 mEq/L. Thus a low-normal HCO3- with increased PaCO2 is another way to uncover an additional metabolic disorder. Decreased perfusion leading to mild lactic acidosis would explain the metabolic component.
Interpreting Oxygenation • What is ‘normal’ PaO2? 80-100mmHg is normal • Oxygenation gradually deteriorates during lifeSeveral calculations available for determining ‘normal’ based on patient age. PaO2 = 104.2 - (0.27 x age) • i.e., 30 year old ~ 95 mmHg 60 year old ~ 88 mmHg
Interpreting Oxygenation • P(A-a)O2 difference –Normal is 3-25mmHg • Increased P(A-a)O2 - • Shunt • V/Q mismatch • Diffusion defect
Interpreting Oxygenation Oxygenation index- PaO2 /FiO2 • Normal is 500 • 200-300 is moderate shunt/ V/Q abnormality • <200 severe shunt / V/Q abnormality
PaCO2 Equation: PaCO2 reflects ratio of metabolic CO2 production to alveolar ventilation VCO2 x 0.863 VCO2 = CO2 production PaCO2 = ------------------- VA = VE – VD VA VE = minute (total) ventilation (= resp. rate x tidal volume) VD = dead space ventilation (= resp. rate x dead space volume 0.863 converts VCO2 and VA units to mm Hg Condition State of PaCO2 in blood alveolar ventilation > 45 mm Hg Hypercapnia Hypoventilation 35 - 45 mm Hg Eucapnia Normal ventilation < 35 mm Hg Hypocapnia Hyperventilation
Dangers of Hypercapnia • Besides indicating a serious derangement in the respiratory system, elevated PaCO2 poses a threat for three reasons: 1) An elevated PaCO2 will lower the PAO2 and as a result will lower the PaO2. 2) An elevated PaCO2 will lower the pH 3) The higher the baseline PaCO2, the greater it will rise for a given fall in alveolar ventilation,
Case 3 – Patient with Severe Abdominal Pain
Case 3 – Patient with Severe Abdominal Pain An obese 70 year old man has diabetes of 25 years duration complicated by coronary artery disease (CABG x 4 vessels 10 years ago), cerebrovascular disease (carotid artery endarterectomy 3 years ago) and peripheral vascular disease (Aorto-bifem 2 years ago). [“VASCULOPATH”]
Case 3 – Patient with Ischemic Bowel ABGs obtained in the ICU pH 7.18 PCO2 20 mmHg HCO3 7 mEq/L
Case 3 – Patient with Ischemic Bowel ABGs obtained in the ICU pH 7.18 PCO2 20 mmHg HCO3 7 mEq/L What is the primary disorder? What is the physiologic response to this disorder?
Case 3 – Patient with Ischemic Bowel Step 1: Acidemic, alkalemic, or normal? METABOLIC ACIDOSIS