Procedures
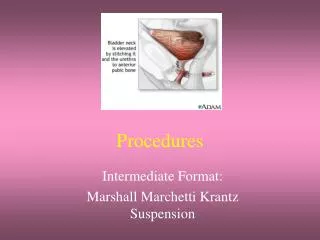
Procedures. Intermediate Format: Marshall Marchetti Krantz Suspension. Objectives. Assess the related terminology and pathophysiology of the MMK. Analyze the diagnostic interventions for a patient undergoing a MMK. Plan the intraoperative course for a patient undergoing MMK.

Procedures
E N D
Presentation Transcript
Procedures Intermediate Format: Marshall Marchetti Krantz Suspension
Objectives • Assess the related terminology and pathophysiology of the MMK. • Analyze the diagnostic interventions for a patient undergoing a MMK. • Plan the intraoperative course for a patient undergoing MMK. • Assemble supplies, equipment, and instrumentation needed for the procedure.
Objectives • Choose the appropriate patient position. • Identify the incision used for the procedure. • Analyze the procedural steps for MMK. • Describe the care of the specimen.
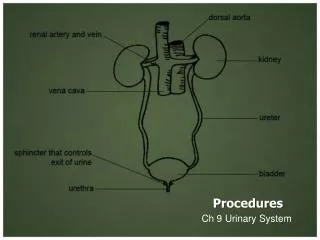
Terms and Definitions • Urinary Incontinence • Stress Urinary Incontinence: inability to retain urine during stress (eg laughing, lifting, sneezing) • Weakened musculature • Urethrocele: pouchlike protrusion of the urethral wall in the female • Cystocele: bladder hernia that protrudes into the vagina
Definition/Purpose of Procedure • Suspension of the bladder to the symphysis pubis to correct stress incontinence • Performed to alleviate stress urinary incontinence
Pathophysiology • Relaxation of pelvic floor leads to stress urinary incontinence.
Diagnostics • Pelvic Exam • Urinary journal • Urinary stress test • Q-Tip test
Surgical Intervention:Special Considerations? Op Preparation • Patient Factors • Room Set-up • Planning: General Anesthesia preferred, pt will be supine w/Trendelenburg, Prep; remove anterior pubic hair, insert Foley, Draping considerations—under-the-buttocks drape, may cut disposable lap sheets to accommodate frog-leg position and provide vaginal access; towel may be used to temporarily cover opening in drape providing vaginal access
Surgical Intervention: Positioning • Position during procedure • Supine w/ Trendelenburg; frog-leg OR • Modified Lithotomy • Supplies and equipment • Allen stirrups or other knee-supporting type • Special considerations: high risk areas (peroneal nerve)
Surgical Intervention: Special (Practical) Considerations/Incision • Special considerations • Extra gloves & maybe an additional gown will be necessary for the assistant—change after providing intravaginal urethral support/vaginal manipulation during suturing • Foley cath may be inserted by circulator during prep or from the sterile field • STSR should be especially aware of potential for contamination of field dur to vaginal and abdominal areas being incorporated in the same drape. • State/Describe incision: Pfannenstiel
Surgical Intervention: Supplies • General: Basic Pack, Double basin, gloves, Blades # 10 x 2, Transverse Lap Drape, Impervious ½ sheet, ESU pencil, NaCl irrigation, ESU extension tip, suction tubing, 4 x 4s, Laps, Kittners or Peanuts • Specific • Suture: • Medications on field (name & purpose) • Catheters & Drains : Foley at beginning of surgery; Possible wound drain • Dressing: possible vaginal packing; 3-layer
Surgical Intervention: Instruments • General: Major instrumentation set • Specific: Long instrument set, Heaney needle holders x 2, several long Allis clamps; self-retaining retractor, hemoclip appliers on standby
Surgical Intervention: Equipment • General: ESU, Positioning Aids • Specific: If modified lithotomy, may need knee-support stirrups and padding
Surgical Intervention: Procedure Steps • Pfannenstiel incision is used to approach the retropubic space • A # 10 blade on # 3 knife handle is uded for incision. Provide cautery and suction. • The bladder and urethra are freed from behind the symphysis pubis using blunt dissection techniques. • Surgeon may use fingers, peanut sponges on a long Mayo clamp, or a sponge on a stick for dissection. Prepare supplies in advance of need.
Surgical Intervention: Procedure Steps Cont’d • The endopelvic fascia is incised to allow for displacment of the bladder. • A # 10 blade on #3 Long knife handle may be needed, according to patients’s size (depth). • Assistant inserts 2 gloved fingers into the vagina to elevate the base of the bladder—to facilitate suture placement and reduce tension. • Protect sterile field from contamination during this process
Surgical Intervention: Procedure Steps Cont’d • Four heavy absorbable sutures are placed in strategic locations in the anterior wall bilaterally to the urethra and are secured in the posterior symphysis or Cooper’s ligament • Load sutures on Heaney needle holders for placement. Anticipate the use of all four sutures sequentially. A series of hemostats may be requested to “tag” the sutures until all have been placed and are ready for tying.
Surgical Intervention: Procedure Steps Cont’d • All sutures are positioned and then tied sequentially for optimum elevation of the bladder • Provide suture scissors as needed. Assist circulator in changing assistant’s gown and gloves as necessary. Provide towel to cover site following bladder elevation. Prepare drain, if requested. Anticipate would closure and prepare suture.
Surgical Intervention: Procedure Steps Cont’d • A wound drain may be placed (eg. Lg penrose) in the space of Retzius. The wound is closed and dressed.. • Count. Provide 3-layer dressing material • Vaginal packing may be inserted to temporarily reduce tension on the suture line. • Vaginal packing is inserted after abdominal dressing is in place.
Counts • Initial; sponges, sharps, instruments • First closing • Final closing • Sponges • Sharps • Instruments
Specimen & Care • Identified as n/a • Handled: routine, etc.
Misc Post –op Info • Immediate Post op Care • Blood tinged urine may be noted in Foley drainage bag • Foley cath may be removed in PACU—the patient is expected to void normally • Prevention: Perform Kegal excercises, limit caffeine intake, which can reduce frequency and urgency, good perineal care; avoid straining & Valsalva Maneuver postop
Prognosis & Complications • Prognosis • 70-95% cure rate • Complications • Hemorrhage (hematuria, excessive vaginal drainage, or incisional), Infection, Recurrence of SUI, increased risk of UTI w/catheter or instrumentation of urinary tract, inability to urinary, new onset of urge incontinence
Other Procedures for SUI • Bladder Neck Suspension • Sling Procedure • Anterior Vaginal Repair/Paravaginal
Resources • Alexander’s p. 587-588 • Goldman pp. 200-202 • Lemone & Burke p. 734, 735, 739, 740, 1566 • MAVCC Info Sheets Unit 5 &Terms & Definitions Unit 6 • STST p. 772 Procedure 20-3 • www.allrefer.com