Download

1 / 87
890 likes | 1.13k Vues
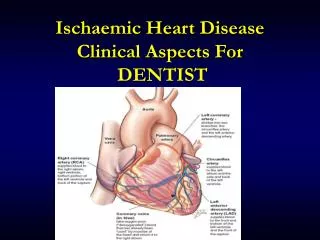
بنام خدا Pharmacology of Ischaemic Heart Disease موضوع امروز ما ایسکمی است ایسکمی باعث درد میشود : آنژین ANTIANGINAL DRUGS. Ischaemic Heart Disease. T he most common cause of death in old males (over 60) Acute: Myocardial Infarction Chronic: Angina pectoris

E N D
بنام خداPharmacology ofIschaemic Heart Diseaseموضوع امروز ما ایسکمی استایسکمی باعث درد میشود :آنژینANTIANGINAL DRUGS
Ischaemic Heart Disease The most common cause of death in old males (over 60) Acute: • Myocardial Infarction Chronic: • Angina pectoris • Silent Ischaemiaبی علامت
Definition Angina = Pain
Definition 3 types of angina: 1. Typical(exertional, classic) • Most common form (90%) • Coronary insufficiency due to vessel occlusion (atherosclerosis) • Attacks usually occur during exercise (climbing stairs, etc.) when oxygen demand exceeds supply
Definition Angina Subtypes (cont.) 2. Variant (Prinzmetal’s) [rest angina] • Coronary insufficiency due to vasospasm • Attacks often occur during rest (e.g., at night) 3. Unstable angina (acute coronary syndrome) • Serious problem • Increased frequency & severity of attacks • Caused by atherosclerotic plaques, & vasospasm
Definition • Typical (exertional, classic) • Variant (Prinzmetal’s) [rest angina] • Unstable (acute coronary syndrome)
Risk Factorsعوامل خطر • Hypertension • Smoking • Hyperlipidaemia ( Cholesterol ) • Hyperglycaemia • Male • Post-menopausal
Risk Factor Atherosclerosis Arteriosclerosis کلسترول یادمان باشد لطفا
Chronic Ischaemic Heart Disease • ANGINA arises as a result of a mismatch between myocardial blood:عدم تعادل • Oxygen supply and demand Attacks of angina precipitates by increases of cardiac work and myocardial oxygen demand کار قلب و تقاضای اکسیژن
Chronic Ischaemic Heart Disease SUPPLYDEMAND زیاد میکند - کممیکند
Oxygen supply Delivery (CBF) *** Extraction *
Oxygen demand Double product: HR X SYST P End Diastolic Tension
The purpose of drug treatmentاهداف درمان • Relieve symptoms: NO PAIN KILLER • Halt the disease process • Prevent myocardial infarction • Prevent death ( % ? )
Drug Therapy کاهشتقاضاوافزایشعرضه • Decreasing myocardial oxygen demand by reducing cardiac workload • Increasing the supply of oxygen to ischemic myocardium • NON DRUG THERAPY
Drug Therapy • Nitrates • Beta-adrenoceptor antagonists • Calcium channel blockers • Potassium channel openers • Aspirin • Cholesterol lowering agents
Nitrovasodilators • GLYCERYL TRINITRATE (GTN) • Sublingual, buccal, transdermal • ISOSORBIDE MONONITRATE AND DINITRATE • Sustained release formulation, tablets پیشگیری یادمان باشد لطفا
Pharmacology • The nitrovasodilators relax almost all smooth muscle by releasing NO which then stimulates the release of cGMP • Onset, Duration of action • Broken by hep. nit. reductase
Nitrate Mechanism (Note: not interact well with actin) From Katzung’s Basic & Clinical Pharmacology 9th ed.
Nitrovasodilators • Venodilation - primary mechanism • There is more enzyme that converts nitroglycerin to NO in venous smooth muscle vs. arterial. • Venodilation results in decreased “preload”(decreased ventricular chamber size, end diastolic pressure, fiber tension) = decreased work ( PARK) • Decreased preload results in decreased O2 demand • Reduction of afterload (arterial resistance) can be produced at higher doses - can produce reflex tachycardia
Nitrovasodilators Additional Mechanisms: 2) Redistribution of coronary blood flow Organic nitrates can selectively increase blood flow to ischemic areas Total coronary flow is not increased 3) A reversal of coronary vasospasm
Nitrates relieve angina by: Arteriolar dilatation reduces cardiac afterload and thus myocardial demand • Peripheral venodilatation reduces venous return, cardiac preload and myocard. work • Relieving coronary vasospasm No evidence that nitrates reduce mortality
Usesموارد استعمال • GTN • Used for the rapid treatment of angina pain. • To avoid first pass metabolism is given by the sublingual route. • May be used frequently and prophylactically • Oral Nitrates • Commonly given as a once a day sustained release formulation • Used for prophylaxis پیشگیری یادمان باشد لطفا
Intravenous nitrates The main stay in the treatment of unstable angina where they are used in combination with heparin
Tolerance تحمل • Tolerance can develop rapidly to the effects of nitrate therapy • Overcome this problem by: • Give doses of nitrate 8 am and 2 pm • Using a sustained release preparation which incorporates a “nitrate free period”
Adverse Drug Reactions (ADR) • Orthostatic hypotension, headache, dizziness, tachycardia (baroreceptor mediated)
Beta Blockers Atenolol • Beta blockers are reversible antagonists of the 1 and 2 receptors • Newer drugs are cardioselective acting primarily on the 1 receptors • These agents block the physiological responses to adrenaline and noradrenaline i.e. the sympathetic system They are N O T VASODILATOR ! ! ! N O T N O T N O T ! ! !
Beta blockers • Beta blockers decrease three major determinants of myocardial oxygen demand • Heart rateکاهش تعداد • Contractilityکاهش زور • Systolic wall tensionکاهش کشش • Beta blockers also allow improved perfusion of of the subendocardium by increasing diastolic perfusion time طولا نی کردن دیاستول مفید است
Beta Blockers: Increase the exercise threshold at which angina occurs
Beta Blockers: Use: • Only forprophylaxis of exertional angina • Ineffective (or contraindicated) for variant angina (may make attacks worse)
Definition • Typical (exertional, classic) (Beta) • Variant (Prinzmetal’s) [rest angina] • Unstable (acute coronary syndrome)
Beta blockers post MI : • Beta blockers are used • in the treatment of acute MIپیشگیری تاکی آریتمی • for secondary prevention in the survivors of an acute MI. • I.V.ATENOLOL or METOPROLOL reduce mortality following an acute MI by 10-15% • Oral beta blockade started weeks or months post MI reduce cardiac death by 22% and second MI by 26%
Rebound Phenomena • محض رضای خدا : قطع نفرمایید • Sudden cessation of beta blocker therapy may precipitate myocardial infarction • Those at risk include patients with angina and men over 50 years receiving beta blockers for other reasons • Rebound beta receptor up-regulation
Contraindicationsلطفا مصرف نفرمایید • Asthmaتنگ نفس بازدمی • Peripheral Vascular Disease • Heart failure • Bradycardia / Heart block
Adverse Drug Reactions • Tiredness /fatigue/lethargy • Impotence • Bradycardia • Bronchospasmباز هم آسم !!! کدام خطرناک تر است ؟
Drug -Drug Interactions • Primarily Pharmacodynamic • Hypotension when used with other hypotensive agents • Bradycardia when used with drugs such as verapamil or diltiazem • Cardiac failure when used with negatively inotropic agents such as verapamil, diltiazem • Exaggerate the hypoglycaemic actions of insulin or oral hypoglycaemics
Calcium Channel Blockers DILTIAZEM, VERAPAMIL, AMLODIPINE • Prevent calcium influx into myocytes and smooth muscle lining arteries and atrerioles by blocking the L-Type calcium channel • Rate limiting CCBs like diltiazem and verapamil also reduce heart rate • CCBs like nifedipine or amlodipine may produce a reflex tachycardia
CCBs reduce vascular tone and so produce vasodilatation • reduce after load and so myocardial work load • CCBs reduce myocardial contractility • reduce myocardial oxygen requirements • CCBs reduce heart rate • reduce myocardial oxygen requirement
Calcium Channel Blockers Mechanism • O2 Demand - probably “most” important • Decreased HR • Decreased contractility • Decreased afterload (TPR, BP) - little effect on venous resistance vs. arterial • Increase coronary blood flow (useful in vasospastic angina)
Contraindications • Evidence that the use of rapidly acting vasodilatatory-CCBs (nifedipine) may precipitate acute MI or stroke • Post MI • May increase morbidity and mortality in patients with impaired LV function • Unstable angina • Evidence that dihydropyridines may increase infarction rate and death in the unstable patient
Adverse Drug Reactions(ADR) • Ankle oedema: Affects 15-20% of patients and does not respond to diuretics • Headache • Flushing • Palpitation
Supply vs. Demand * Nitrates, CCBs, -blockers O2demand Normal balance O2delivery Angina Nitrates, CCBs, Revascularization * More often, drugs are used to decrease O2 demand
Potassium Channel Openers NICORANDIL • Activate “silent” potassium channels • The entry of potassium into cardiac myocytes inhibits the calcium influx and so has a negative inotropic action
Antiplatelet Agents • Low dose ASPIRIN (75-150 mg) • The formation of platelet aggregates are important in the pathogenesis of angina, unstable angina and acute MI • Aspirin is a potent inhibitor of platelet thromboxane production • Thromboxane stimulates platelet aggregation and vasoconstriction
Cholesterol Lowering Agents SIMVASTATIN, PRAVASTATIN, ATORVASTATIN • HMG CoA Reductase Inhibitors and the most effective cholesterol lowering agents • Reduces cardiovascular mortality by 42% and total mortality by 30%
Non Pharmacol. Therap. No risk factors No smoking Moderate physical activity سخت نگیرEasy life
New mechanistic approaches to myocardial ischemia • Rho kinase inhibition (fasudil) • Metabolic modulation (trimetazidine) • Preconditioning (nicorandil) • Sinus node inhibition (ivabradine) • Late Na+ current inhibition (ranolazine)
Rho Fasudil Rho kinase Rho kinase inhibition: Fasudil Rho kinase triggers vasoconstriction through accumulation of phosphorylated myosin Agonist Ca2+ Ca2+ Receptor PLC PIP2 VOC ROC IP3 SR Ca2+ Myosin Myosin phosphatase MLCK Ca2+ Myosin-P Calmodulin Adapted from Seasholtz TM. Am J Physiol Cell Physiol. 2003;284:C596-8.
O2 requirement of glucose pathway is lower than FFA pathway During ischemia, oxidized FFA levels rise, blunting the glucose pathway Metabolic modulation (pFOX): Trimetazidine Myocytes Glucose FFA Acyl-CoA Pyruvate β-oxidation Trimetazidine Acetyl-CoA Energy for contraction MacInnes A et al. Circ Res. 2003;93:e26-32. Lopaschuk GD et al. Circ Res. 2003;93:e33-7. Stanley WC. J Cardiovasc Pharmacol Ther. 2004;9(suppl 1):S31-45. pFOX = partial fatty acid oxidation FFA = free fatty acid
Do you need O2 ? صرفه جويي كن !!!1. معمولا قلب براي توليد انرژي چربي ميسوزاند (كلي اكسيژن ميبرد)2. اكر نشد ميتواند گلوكز بسوزاند كه خيلي كمتر اكسيژن ميبرد .3. در مسير چربي سوزان يك آنزيم مهم است: بتا اكسيداز ميتوكندريايي4. آيا ميتواني دارويي بسازي كه اين مسير را ببندد؟5. بله !!