Download
1 / 20
200 likes | 337 Vues
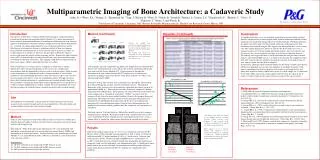
PANARAB’12. NR28. IMAGING OF DYSEMBRYOPLASTIC NEUROEPITHELIAL TUMORS. A STUDY OF 6 CASES. Amina EL KHAMLICHI * , Meriem FIKRI*, Yasser ARKHA**, Najoua ECH-CHERIF EL KETTANI*, My Rachid EL HASSANI * , Abdeslam EL KHAMLICHI ** , Mohamed JIDDANE *. * Department of Neuroradiology

E N D
PANARAB’12 NR28 IMAGING OF DYSEMBRYOPLASTIC NEUROEPITHELIAL TUMORS. A STUDY OF 6 CASES Amina EL KHAMLICHI*, Meriem FIKRI*, Yasser ARKHA**, Najoua ECH-CHERIF EL KETTANI*, My Rachid EL HASSANI*, Abdeslam EL KHAMLICHI**, Mohamed JIDDANE* *Department of Neuroradiology **Department of Neurosurgery Hôpital des Spécialités, CHU Ibn Sina, Rabat, Morocco
Introduction • DysembryoplasticNeuroepithelialTumors (DNTs) include a large morphologicalspectrum of tumorswhichhistologically resemble gliomas but are carcinologically perfectly stable lesions. Thesetumors are seen in young patients withintractable partial epilepsy. • The purpose of thisstudyis to evaluate CT and MRI features of dysembryoplasticneuroepithelial tumors .
Materials and methods • Our studyconcerns 6 cases of dysembryoplasticneuroepithelial tumorshistopathologically confirmed and diagnosed in patients who underwent corticectomiesbetween 1998 and 2011.
Materials and methods • Clinical symptoms : • Grand mal epilepsy (n = 2) • Pharmacoresistant partial seizures (n = 3) • Absence seizure (n = 1) • Symptoms beginning : * before age of 20 years : n = 4 * after age of 20 years : n = 2 • Symptoms of raised intracranial pressure (n = 1) • Neurological deficit (n = 0)
Materials and methods • All patients underwentbrain MRI and CT. • CT examinationincluded axial and coronal sections before and aftercontrast administration. • MRI examinationincluded T1 and T2 axial, sagittal and coronal sections bothpre- and postcontrast. FLAIR werealsoutilised.
Materials and methods • Studiedparameters : • Location and topography • Signal on T1, T2 • Contrastenhancement • Calcifications and cystic component • Size • Limits • Mass effect • Peritumoraledema
Results • In all cases a single focal supratentoriallesion on CT and MRI examinations • Location :* Temporal lobes (67%) : right (n = 3) and left (n = 1) * Right posterior parietal lobe (n = 1) * Left frontotemporal lobe (n = 1) Case 5 Case 6 Case 4 Case 3
Results • CT scan :*Hypodenselesion (n = 6) * ± Calcifications (n = 3) * Non-enhancing tumor or faint enhancement of solid portion. Case 2 Case 1 Case 4
Results • MRI :* Hypointense on T1-WI (n=6) *Hyperintense on T2-WI and Flair images (n=6) Case 2 Case 6
Results • Contrastenhancement :*Ring shaped (n = 3) * Nodular pattern (n = 2) * No enhancement (n = 1) Case 6 Case 4 Case 5
Results • Lesion pattern :*Pseudocystic, multilobulated (n=5) Case 6 Case 5 Case 4 Case 3
Results • Mass effect : Minimal (n = 2), absent (n = 4) • Peritumoral edema:Minimal (n = 1), absent (n = 5) Case 2 Case 3 Case 4
Discussion • 0.4 – 1.3 % of all braintumors Histopathology : • Specific glioneuronalelement : columnar structure made up of bundles of axons lined by small tumoral oligodendrocytes. • 3 histologicalforms : * simple : a unique specificglioneuronalelement * complexe : - a specificglioneuronalelement - a multinodular architecture - foci of cortical dysplasia * non specific : no specificglioneuronalelement or multinodular architecture
Discussion Imaging Threeradiological features of DNT, not sensitive and not specific, are helpful for the diagnosis : • cortical topography • no « digit like » peritumoraledema • no mass effect CT scan: • Well-circumscribedhypodenselesion, whichusuallyappears as non enhancing mass ± Focal enhancement in 21 % of cases ± Calcifications in 36 % of cases ± Pseudocystic aspect in 50 % of cases ± « Scalloping » • Brain CT wasreported as normal in 10 % of cases (isodensesmalllesion)
Discussion MRI +++: • T2 Weighted Images +++ • Tumortopography : cortex and/or subcortical white matterinvolvement • Hypersignal on T2 WI: 100 % • Polymorphic aspect : « nodular » (77%) or « megagyri » configuration (23%) • Tumor size : 8 – 60 mm • Microcystic pattern iscommon : « soap bubbles » appearance • Truecystis rare (7%) [size less to 1 cm]
Discussion Imaging featuresaccording to the histologicallyforms : • Simple form pseudo-cystic, welldelineated, homogenous appearancewith no calcifications or any enhancementaftercontrastexamination • Complexe form ring-likecontrastenhancement, calcifications • Non specificformnodularenhancement, « megagyri » pattern, calcifications
Discussion Positive diagnosis : The diagnosis of DNT must be considered when the following criteria are associated : • MRI : intracorticallesionwith no mass effect and no peritumoraledema • Histological featureresemblegliomas but withoutlymphocyticinfiltrates • Partial seizureswith or without secondary generalization • Symptomsbeginningbefore 20 years of age • No neurologicaldeficit or stable congenitaldeficit Differentialdiagnosis: *Ganglioglioma *Low grade oligodendroglioma
Discussion Follow-up : *DNTs are carcinologically stable lesions * Absence of recurrencesafter total resection In ourstudy, the meanfollow-up was 21 months. One patient developedtumorrecurrenceappeared 2 yearsafterincompleteprimaryresection
Conclusion • DNTs is a recently defined category of tumors in young patients. These tumors histologically resemble gliomas but behave as stable lesions. MR imaging allows a better knowledge of their characteristic imaging features. • Three radiological features of DNT are helpful for the diagnosis: cortical location, absence of mass effect and no peritumoral edema.
References • StanescuCosson R, Varlet P, Beuvon F, DaumasDuport C, Devaux B, Chassoux F, Frédy D, Meder JF. Dysembryoplasticneuroepithelialtumors: CT, MR findings and imaging follow-up: a study of 53 cases. J. Neuroradiol., 2011;28 : 230-240 • Daumas-Duport C, Varlet P, Bacha S, Beuvon F, Cervera-Pierot P, Chodkiewicz JP. Dysembryoplasticneuroepithelialtumors: nonspecifichistologicalforms – A study of 40 cases. Journal of Neuro-Oncology, 1999; 41 : 267-280 • Daumas-Duport C, Scheithauer BW, Chodkiewicz JP, Laws ER,Vedrenne C. (1988). Dysembryoplasicneuroepithelialtumor: a surgically curable tumor of young patients with intractable partial seizure. Report of thirty-nine cases. Neurosurgery, 23: 545-556 • El Kettani N, Sqalli-Houssaïni N, Sbihi S et al. Tumeur neuroépithélialedysembryoplasique. Feuillets de Radiologie 2007;47(1):46-51 • Litrico S, Desjardins T, Dran G et al. Localisation sous-tentorielle d’une tumeur dysembryoplasiqueneuroépithéliale. Neurochirurgie 2004;50(1):47-52 • Rodrigo S, Chassoux F, Oppenheim C, Devaux B, Méder JF. Nouvelle approche sémiologique en IRM des tumeurs dysembryoplasiquesneuroépithéliales. Journal de Radiologie, 2006; 87(10), Page 131 • Ben Yaacoub I, Sebai R, Hammami N, Belghith L, Bellakhal J, Nagi S, Ben Hammouda M. Apport de l’imageriedans le diagnostic des tumeursdysembryoplasiquesneuroépithéliales: à propos de 11 cas. Journal de Radiologie, 2007; 88(10), Page 1554