Short Stature
Short Stature. PLEAT Endocrinology 8/7/2011 Nadia Muhi Iddin Conquest hospital. Definitions. Short stature describes the lower end of a height distribution for a given population. It is not necessarily indicative of abnormality.

Short Stature
E N D
Presentation Transcript
Short Stature PLEAT Endocrinology 8/7/2011 Nadia Muhi Iddin Conquest hospital
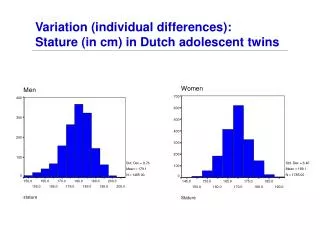
Definitions • Short stature describes the lower end of a height distribution for a given population. It is not necessarily indicative of abnormality. • Height charts illustrate action levels outside which a child’s height warrants a more detailed evaluation. • UK growth charts a specific action threshold for 0.4 and 99.6. The 0.4 equates to -2.67 SD. Only 1 normal child in 260 has a height below this line. • Children with a height below2nd centile 2SD.
Definition • Short stature, optimally defined relative to the genetic endowment of the individual, is recognized by comparing an individual child’s height with that of a large population of a similar genetic background and, more particularly, using the mid-parental target height.
History. Short stature? cause • Pregnancy ,birth and neonatal history and weight. • Current health & nutritional status/ diet. • Parent held record. School record or health record. • Parental height and onset of puberty. • Consider environmental and emotional deprivation.
Failure to Thrive ( Faltering growth) • Overlap. • Childs 1st year or two with unsatisfactory weight gain and growth ( length). Causes of growth failure • Prenatal: • Chromosomal, genetic ,skeletal, infectious, syndromic. • Neonatal: Organ and systemic disorders and malnutrition. • Childhood :Familial, social ,systemic, endocrine. • Adolescence: Constitutional delay of growth and puberty. Hypogonadism
Causes of faltering growth • Inadequate food intake. • Feeding problems, neglect, poor appetite ,mechanical • problems, cleft palate, Cerebral Palsy. • Vomiting: GI reflux, Pyloric stenosis, food intolerance • Defects of digestion and absorption: CF, Coeliac disease, • Chronic diarrhoea • Failure of utilisation: Heart failure, metabolic disorders. • Emotional deprivation
Measurement • Appropriate for age. • Trained staff. • Accurate plotting on growth charts.
Child health Surveillance Current recommendations:
SCHOOLS AND ACTIVITIES Schools, play groups, etc., are sometimes unaware of the problems that children who are very small for their age have to deal with such as practical difficulties of being unable to reach a peg or desk or sit on the toilet. They may also experience psychological problems of not being accepted by friends of the same age or being treated like a toy and picked up by other children. (This problem is not only an annoyance but also means physical danger. Serious accidents have occurred when children are carried inappropriately in the playground.) It may be advisable to visit your child's school or play group to discuss your child's condition as this can help teachers and carers to plan the support and avoid problems before they arise. If problems do occur, and you feel unable to cope, contact the CGF who will put you in touch with other parents with similar problems who may be able to give practical help and support. If the problem becomes more severe, help may be available from an educational psychologist from the school or a child psychiatrist in association with your specialist growth centre. Most of us tend to adjust our expectations for a child that looks younger and sensible discussion of this problem can help to counteract this natural tendency and ensure that your child is treated in a manner appropriate to his/her age.
Specialist advice on short stature is needed when: • Single height measurement below 0.4th centile • Associated signs & symptoms that suggest a health disorder. • Family concern. • Height crossing two centiles or a complete channel. This allows growth failure to be identified even though a Childs height is still above the 2nd centile.
The foetal & infantile phase are mainly dependant on adequate nutrition
Pathological short stature • Defects of nutrition ,digestion or absorption. • Most malformation syndromes. Downs, Noonan’s, Russell Silver • Chronic disease. Renal failure, Malignancy, Crohn’s, CF. • Turner syndrome and variants. • Hypothyroidism • Long term steroid therapy, Cushing’s syndrome is very unusual in childhood • Bone disorders. Skeletal dysplasia. Check sitting height. • Growth hormone disorders. Isolated or secondary to pan-hypopituitarism. • Social and emotional deprivation. • Endocrine are uncommon causes. They are associated with children being • relatively overweight.
Examples Septo-optic dysplasia. • Absent septum pellucidum. • Optic nerve aplasia or hypoplasia. • Pituitary gland hypoplasia /dysfunction. Growth hormone insensitivity syndrome ( Larone’s syndrome). GH levels frequently very high and children untreatable.
Turner’s Syndrome • 1/2500 live births • Most common Karyotype is 45X0. • Mosaicism as 45X/46XX,45X/46XY,45X/47XXX. • Most consistent feature is short stature and gonadal dysgenesis. • All short girls should have their Karyotype checked. • No growth hormone deficiency.
Investigations for Short stature • Full blood count. ESR, Iron levels. • Urea ,electrolytes and. Ca profile, Liver function • TSH and possible LHRH, TRH test • CRP, Transglutaminase Ab test • Radiology: Bone age, US, Skeletal survey, Echo. • Chromosomes in females or if needed. • Dynamic Growth hormone provocation test ( Insulin tolerance, Glucagon stimulation ,arginine).
Indications for treatment Pit-hGH was withdrawn in 1985 when a number of treated patients developed Creutzfeldt-Jakob disease (CJD). In the same year the first biosynthetic hGH (met-hGH, somatrem) became available in the UK, followed by natural sequence r-hGH (somatropin) in 1988. All GH used in the UK is now r-hGH, manufactured using E-coli or mammalian vectors and is structurally, chemically and biologically identical to pituitary-source hGH. GH currently has a product licence in the UK for the following conditions: • GH-deficiency (GHD): paediatric and adult licences. • Turner syndrome (TS) • Chronic renal insufficiency (CRI) • Prader-Willi syndrome (PWS) • Small for gestational age (SGA) New Indications.
NICE Guidelines The first four paediatric indications were included in the NICE technology assessment of May 2002 and have been ratified. The SGA licence was not granted until 2003 (i.e.. after the NICE review) and is likely to be dealt with in the subsequent NICE review (due 2007-8). Absence of NICE guidance is not, however, a reason for refusing GH therapy for licensed indications. Jane Kennedy MP, Minister of State for Quality and Patient Safety stated, on 7 December 2005 at the NICE Conference: 'It is not acceptable for the local NHS to cite a lack of NICE guidance as the sole reason for not providing a treatment. A key role of the NHS has been, and will continue to be, to make decisions about the use of new pharmaceuticals. NICE does not exist to “kite mark” all the drugs which are licensed for use in the UK.
LICENSED INDICATIONS • Growth hormone deficiency (GHD) • GHD is the commonest endocrine disorder presenting with short stature; it is estimated that • 25% of children with a height < -3 SDS have GHD. The frequency of GHD is estimated at 1 • in 3,500-4,000, although a milder phenotype may occur in up to 1 in 2,
Who can have human growth hormone (somatropin)? • growth hormone deficiency • Turner syndrome • Prader–Willi syndrome • chronic renal insufficiency • growth failure at 4 years or older and were born small for gestational age • short stature homeobox-containing gene (SHOX) deficiency. review plans for this guidance in May 2013
Human growth hormone (somatropin) for the treatment of growth failure in children (review) Issued: May 2010 Description NICE recommends human growth hormone (somatropin) as a possible treatment for some children with growth failure (see below). Who can have human growth hormone (somatropin)
BSPED Guidelines for management • Below is a model for managing relatively common endocrine disorders and those deemed to be more complex: • Level 1: Conditions with a low level of anticipated need for input from a paediatrician with an interest in endocrinology - • managed in most cases by local general paediatricians: • Familial short and tall stature children • Nutritional obesity • Level 2: Conditions with a need for input from a paediatrician with an interest in endocrinology usually managed at local DGH clinics with occasional input from a paediatric endocrinologist at regional level on a shared care basis with the local • teams. For some conditions the initial diagnostic investigations may need to be undertaken at the lead centre. • Above conditions • Primary hypothyroidism (congenital and acquired) • Delayed puberty in boys • Variations of early pubertal development in girls • Vitamin D deficiency
BSPED guidelines for management 2 • Level 3: Conditions which require all or some management from a paediatric endocrinologist at regional level. These • conditions are managed solely by a regional unit or through a network of endocrine clinics at the DGH, performed in • combination by a regional paediatric endocrinologist and a local paediatrician with an interest in endocrinology. Some • conditions that require MDT input from a number of specialists through joint clinics at regional or supra-regional level will • require attendance at specialist centres for some of their visits. • Anterior and Posterior Pituitary hormone deficiency • Complex midline defects e.g. Septo Optic Dysplasia • Delayed puberty in girls • Endocrine abnormalities associated with chromosomal disorders e.g. Turner syndrome, Klinefelter syndrome, • Prader Willi syndrome. • Cushing’s syndrome • Skeletal dysplasia's • Endocrine tumours including familial forms • Endocrine Disorders Associated with Chronic Disease • o Growth and pubertal problems associated with chronic renal failure • o Care of endocrine problems in cancer survivors • Inflammatory conditions such as inflammatory bowel disease, arthropathies and other connective • tissue disorders • Planning of transition to adult services • It is vital that close relationships exist between paediatric and adult endocrinology services
Treatment of Children with Recombinant Human Growth Hormone (r-hGH) Shared Care Guidelines April 2006 Jeremy Kirk & Gary Butler on behalf of the British Society for Paediatric Endocrinology and Diabetes (BSPED) SHARED CARE of PATIENTS on GH THERAPY Background Although linear growth is influenced by a number of factors, growth hormone (GH) plays a predominant role with both direct and indirect effects on the epiphyseal growth plate. It also affects carbohydrate and lipid metabolism, nitrogen metabolism and tissue growth. Pituitary extracted growth hormone (pit-hGH) was first used as a treatment for growth hormone deficiency (GHD) in children in l958. As supplies were reliant on the availability of cadaveric pituitaries, only the most severely affected children were treated using standard doses e.g. 4 U (1.3 mg) thrice weekly by intra-muscular. injection.
UK-WHO growth charts: early years • The new UK-WHO Growth Charts for children from birth to 4 years of age are now available. The charts have been developed as a project undertaken within the Science and Research Department led by Professor Charlotte Wright from the University of Glasgow and funded by the Department of Health.
The charts are available in an A4 format and has 6 separate charts for insertion into the Personal Child Health Record (PCHR). There is also a new Neonatal and Infant Close Monitoring chart (NICM) (previously referred to as the Low Birth weight chart) to be used for I) births before 32 weeks gestation, ii) unwell neonates born after 32 weeks and iii) for term infants with significant growth and weight faltering. These charts are available in A4 and PCHR format.Phase Two of this project has started to develop new 4-18 years Growth Charts, please check these pages for further updates.
Patterns of growth Ref. Medscape: Robert J Ferry 2010
Left hand and wrist Bone age investigation
Prognosis Growth hormone deficiency • Historical GHD untreated groups have an untreated final height (FH) of 134 –146 cm in males and 128 –134 cm in females. • With GH treatment FH is improved by 8.7 –10.7 cm in boys, & 7.7 – 9.5 cm in girls.
References • THE CHILD GROWTH FOUNDATION (Charity No 274325) 2 Mayfield Avenue Chiswick London W4 1PW 020 8994 7625 & 020 8995 0257 The CGF supports groups within the foundation which deal with specific conditions. The Growth Hormone Group has a voluntary organiser who is available to help with queries or problems relating to Growth Hormone Deficiency. • BSPED Information. • NICE Guidelines • Lecture Notes on paediatrics. R. Medow/S. Newel • Illustrated textbook of Paediatrics. T. Lissaure/G. Clayden • MRCPCH Mastercourse Volume 2