SHORT STATURE
SHORT STATURE. CATALINA RUIZ, MD PL1 SBH. 11/18/10. OBJECTIVES. Definition Growth physiology Evaluation: History, PE, growth chart Etiology Laboratory Growth hormone therapy. SHORT STATURE. DEFINITION


SHORT STATURE
E N D
Presentation Transcript
SHORT STATURE CATALINA RUIZ, MD PL1 SBH 11/18/10
OBJECTIVES • Definition • Growth physiology • Evaluation: History, PE, growth chart • Etiology • Laboratory • Growth hormone therapy
SHORT STATURE DEFINITION • Analysis of the child’s height in the context of expected genetic potential conferred by the parents • Child’s growth curve is crossing percentiles • Child’s growth rate is < 5cm/year • Height is >2 SD (10cm) below from the midparental height.
MIDPARENTAL HEIGHT: GIRLS: (father’s height – 13) + mother’s height /2 BOYS: Father’s height + (mother’s height + 13)/2 The parents height are in cm • TARGET HEIGHT: Midparental height +/- 2SD (10cm)
FAILURE TO THRIVE: Impairment in weight gain greater than linear growth. Can be associated with short stature or slow growth velocity.
PHYSIOLOGY Growth depends on: • Genetic • Nutritional: calories, protein, calcium, minerals, vitamins • Hormones: GH, ILGF- I, thyroid, insulin, sex steroids, glucocorticoids • Others: absence of toxins, adequate sleep, exercise, psychosocial factors.
PHYSIOLOGY • GH PRIMARY CONTROLLERS: • Growth Hormone Releasing Hormone (GHRH) • Somatostatin or somatotropin release inhibiting hormone (SRIH) • Ghrelin
FETAL GROWTH : maternal factors (placental sufficiency, nutrition), insulin and IGFBP. • GROWTH IN LATE INFANCY AND CHILDHOOD: GH/IGF- I axis, thyroid hormone, nutrition and insulin. IGF- I and IGFBP- 3 levels are low during the first 5 years of life.
During the first 3 years children are adjusting to their genetic potential, is normal to see shifts in the growth curve. • First 3 years: 25cm/year 12cm/year 8cm/year • Then: 4-7cm/year Small linear growth deceleration often is seen before the onset of puberty
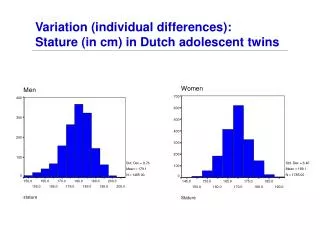
PUBERTAL GROWTH: sex hormones as well as GH/IGF –I axis and thyroid gland. The pubertal growth spurt in girls occurs approximately 2 years earlier than in boys. Peak velocity is slower in girls (8.3cm/y) than in boys (9.5cm/y). This factor combined with a 2 year longer duration of growth in boys, results in an average 13cm difference in adult height between the 2 sexes.
EVALUATION • HISTORY • PHYSICAL EXAM • GROWTH CURVE • BONE AGE (BA) • BODY PROPORTIONS
1.HISTORY • Birth history • Development • Nutrition • Medications • General health • Age of pubertal development • Significant medical events (illnesses, head Tx, Sx) • Activity/exercise • Family history: parents and siblings heights, age of onset of puberty, history of consanguinity, congenital anomalies
2.PHYSICAL EXAM • Facial appearance and apparent maturation, abnormal facies • Dysmorphic features • Skin: birth marks, acne, hair • Body proportions • Hands: short metacarpals, palmar creases • Chest: widely spaced nipples, pectus excavatum, shield shape chest
2.PHYSICAL EXAM • Breast development • General examination (lungs, heart, abdomen, neuro) • Genitalia: Female: pubic hair stage, clitoris size, labia, vagina, estrogen effect. Male: pubic hair stage, genital stage, including phallic and testicle length (>2.5cm max. length signifies entry into puberty)
3. GROWTH CURVE Is the most important step. Consider: • Reliability of measurements • Absolute height • Growth velocity: accurate determination requires at least 3 and preferably 6 months • Weight for height ratio: it has some diagnostic value in identifying the cause of growth retardation in a short child.
4. BONE AGE Gives a level of bone maturation based on centers of ossification and closure of epiphyses. The method most commonly used to asses BA is that of Greulich and Pyle, which examines epiphyseal maturation of hand and wrist
5. BODY PROPORTIONS The U/L ratio indicates whether the short stature is proportionate or disproportionate. It varies with age and race. The lower segment: from the upper border of the symphysis pubis to the floor in a standing patient. The upper segment: subtracting the lower segment from the standing height.
U/L RATIO: 1.7 at birth 1.4 at 2 years 1 at 10 years 0.9 at adulthood Skeletal dysplasia involving primarily the spine (spondylodysplasia) are often associated with decreased U/L ratio for age. Those dysplasia involving especially the long bones (achondroplasia) frequently are associated with increased U/L ratio.
5. BODY PROPORTIONS • Arm span is approximately equal to height in children > 8 years. Can be used as a surrogate for height measurement and for monitor of growth velocity in children who have spina bifida, or leg contractures or after spinal irradiation.
ETIOLOGY • NORMAL GROWTH PATTERNS: Normal growth velocity in a short child • Familial short stature: Normal growth velocity, normal timing of development of puberty, and bones fuse at the appropriate age. Height is short because of short mother and/or father. BA=CA. • Constitutional delay of growth and puberty: Normal or near normal growth velocity, delayed timing of puberty, delayed BA. Family history of late bloomers.
ETIOLOGY • Pathologic causes of short stature • Proportionate short stature with increased weight for height ratio: (deceleration of linear growth in a well nourished or obese child) Endocrinopathy should be suspected, such as hypothyroidism, glucocorticoid excess and GH deficiency.
GHD: congenital or acquired and can be associated with other pituitary defects. Congenital can be related to perinatal asphyxia or associated with embryologic malformations (CNS, midface abnormalities). Acquires occurs most commonly as idiopathic diagnosis, but may result from tumors, head Tx, CNS infections, irradiation, Sx. The child has short stature, slow growth velocity, delayed BA, low IGF-I and IGFBP-3 values.
GH insensitivity: autosomal recessive. Caused by defects in the GH receptor. Phenotype similar to GHD, but biochemically increased GH levels, low IGF-I, IGFBP-3 and GHBP. • Hypothyroidism: if untreated the growth velocity is slow and BA is delayed relative to CA. • Glucocorticoid excess: usually iatrogenic, but also tumors. Growth velocity is slow, BA delayed, weight gain and hypertension.
ETIOLOGY • Proportionate short stature with decreased weight for height ratio: (deceleration of linear growth in a thin child) Systemic diseases, most common undernutrition or malnutrition. With restoration of adequate nutrition, growth usually accelerates (catch up). Also inflammatory bowel disease, celiac disease, kidney disease.
ETIOLOGY • Disproportionate shortening and dysmorphic features: genetic or syndromic causes of short stature. • Skeletal dysplasia: abnormal U/L ratio, BA=CA.
LABORATORY • GENERAL SCREENING TESTS: CBC with diff. BMP, UA, BA, TSH, T4, IGF-I (if >5 years) • SPECIALIZED TESTS: Karyotype, growth hormone stimulation test, dexamethasone suppression test.
GROWTH HORMONE STIMULATION TEST ENDOCRINOLOGY A GH level by itself is meaningless in the evaluation of short stature. Provocative agents include clonidine, L-dopa, arginine, insulin, glucagon, and GHRH. Fasting 8-12 hours 5 blood samples: the first is between 6 and 8 am, then the provocative agent is injected, 30 minutes after that another blood sample, continue every 30 minutes. Normal GH peak value (pass): >8ng/ml
GROWTH HORMONE THERAPY • FDA approved indications for the use of GH GHD Turner syndrome Renal insufficiency Prader Willi syndrome SGA Idiopathic short stature (predicted target height in girls < 4’11; boys <5’3.)
GROWTH HORMONE THERAPY • Administration and dosage: Subcutaneous injection starting at 0.3mg/kg/wk given 6-7 days/wk. • Adverse effects: slipped capital femoral epiphysis, glucose intolerance/diabetes, pseudotumor cerebri, scoliosis.