Download

1 / 85
880 likes | 1.39k Vues
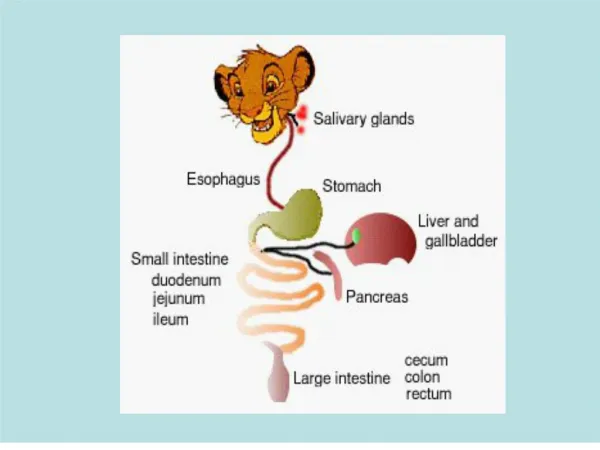
GASTRO- INTESTINAL PATHOLOGY . ESOPHAGUS. Location: posterior mediastinum Distensible muscular tube 23-25 cm in length Upper esophageal sphincter & lower esophageal sphincter Mucosa, submucosa, muscularis propria Transports food & liquids from pharynx to stomach.

E N D
ESOPHAGUS • Location: posterior mediastinum • Distensible muscular tube • 23-25 cm in length • Upper esophageal sphincter & lower esophageal sphincter • Mucosa, submucosa, muscularis propria • Transports food & liquids from pharynx to stomach
Atresia = noncanalized segment of esophagus Fistula = connection between esophagus & trachea ESOPHAGUS: CONGENITAL ANOMALIES & CONSTRICTIONS • Hazards: • aspiration, pneumonia & suffocation
Webs: Upper esophageal mucosal narrowings Plummer-Vinson/ Paterson- Brown-Kelly synd Perimenopausal female + anemia + glossitis risk esophageal ca Schatzki’s rings: Lower gastro-esophageal junction narrowings ESOPHAGUS: CONGENITAL ANOMALIES & CONSTRICTIONS • Webs & Rings: Main Sx: dysphagia • Uncommon, mid age women of unknown etiology • Ledge- like mucosal protrusions
MC acquired (MCC: GE reflux, chemical injury, scleroderma, & radiation injury)
ACHALASIA • Aperistalsis, failure of relaxation of LES & inc resting tone of LES dysphagia, regurgitation, & esophageal dilatation • Predisposes to: • Aspiration pneumonia • Candida esophagitis • Diverticula • Ca (~ 5%) • MC is primary (neuronal degeneration): in young adults, remains for life
ACHALASIA • 2o achalasia: • Chagas’ dse (T. cruzi) • Lesions of vagal motor nuclei • Diabetic autonomic neuropathy • Infiltrative disorders • Morphology: progressive esophageal dilatation above LES, & diminished myenteric ganglia
Upward protrusion of part of stomach through diaphragmatic (esophageal) hiatus Clinically: Affects up to 20% of adults <10% symptomatic Complications: Reflux esophagitis Ulceration Bleeding Perforation HIATAL HERNIA
Sliding hiatal (>90%) px stomach slides through a widened hiatus Rolling/ paraesophageal (<10%) part of stomach (fundus) herniates alongside esophagus into thorax, vulnerable to strangulation, may be caused by previous sx HIATAL HERNIA patterns:
MALLORY-WEISS SYNDROME • Lacerations at GE junction • 2o episode of excessive vomiting + spasm of LES • MC in alcoholics • Clinical: 5-10% of UGI bleeding • Mallory-Weiss tears hematemesis • Morphology: irregular longitudinal tear in EG junction. May involve only mucosa, or may rarely penetrate wall • Tear penetrates all layers (Boerhaave’s synd) mediastinitis or peritonitis
ESOPHAGEAL VARICES • Collateral bypass channels in lower part of esophagus between branches of left gastric vein & azygos veins • Seen in long-standing portal HPN (alcoholic cirrhosis- 90%) • Morphology: Tortuous, dilated veins w/in submucosa of lower esophagus, raising the mucosa & tend to rupture
ESOPHAGEAL VARICES • Clinically: • Asymptomatic until rupture catastrophic bleeding (hematemesis & melena) • Rarely subsides spontaneously • 40-50% fatality rate for each episode of bleeding • 90% chance of recurrence in survivors
ESOPHAGITIS • Incidence: 5% adults (US), 80% (Iran) • Predisposing Factors: • Reflux of gastric contents (reflux esophagitis) • Infections (immunosuppressed patients) • Ingestion of irritants: alcohol, hot tea, smoking • Uremia • Ca chemotx, Radiotx • Prolonged gastric intubation • Systemic desquamative disorders: pemphigoid • GVH dse
Clinical Features 24 hr pH studies: pH <4 > 4.5% of the time Predisposing factors: LES tone, hiatal hernia Heartburn & regurgitation Hematemesis or melena Strictures dysphagia Barrett’s esophagus Morphology: Hyperplasia Elongation of papillae Intraepithelial eos Ulceration & hge in severe cases REFLUX ESOPHAGITIS