Download
1 / 64
640 likes | 805 Vues
Progesterone Supplementation and Prevention of Preterm Birth. Catherine Y Spong, MD Chief, Pregnancy & Perinatology Branch National Institute of Child Health & Human Development National Institutes of Health. Conflict of Interest Statement.

E N D
Progesterone Supplementation and Prevention of Preterm Birth Catherine Y Spong, MD Chief, Pregnancy & Perinatology Branch National Institute of Child Health & Human Development National Institutes of Health
Conflict of Interest Statement • I have no conflict of interest related to the content of this presentation
Objectives • to describe the problem of prematurity • to describe the mechanism of progesterone action • to define the patient population who meets the criteria for progesterone administration to prevent preterm birth
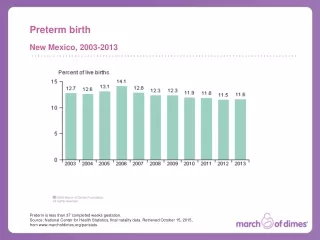
Preterm Delivery: A Public Health Priority • 1 in 8 infants is born preterm • 542,893 preterm births each year (2006) • leading cause of hospitalization among pregnant women • leading cause of death among African-American infants • associated with developmental disabilities
Leading Causes of Neonatal Mortality, 2001 (N / 100,000 live births) 4,322 3,875 1,491 998 • Leading cause of black infant mortality • Second leading cause of all infant mortality 943 http://www.cdc.gov/nchs/data/nvsr/nvsr52/nvsr52_09.pdf Table H. Deaths and percentage of total deaths for the 10 leading causes of neonatal and postneonatal deaths: United States, 2001
Preterm Birth: Outcome • 1 out of 5 children with mental retardation • 1 out of 3 children with vision impairment • Almost half of children with cerebral palsy Accounts for
Preterm Birth: Long Term Outcome • For the baby: • Increased risk for cardiovascular disease (MI, stroke, hypertension) as an adult • Increased risk for diabetes as an adult • Possible increase in cancer risk • For the mother: • Increased risk for subsequent preterm delivery Birth Weight and Coronary Heart Disease Lower BW=higher CHD risk Age Adjusted Relative Risk Birthweight (lbs) Rich-Edwards 1997
Progestins • Steroid hormone • Exogenous or synthetic forms of progesterone • Produced by corpus luteum, adrenals, placenta • Maintains pregnancy • Exerts biologic effects on • Immune response • Myometrium • Chorioamniotic membranes • Cervix
Actions • Delays cervical collagen degradation • Myometrial: • Decreases conduction of contractions • Increases threshold for stimulation • Decreases spontaneous activity • Decreases number of oxytocin receptors • Prevents formation of gap junctions
Progestin formulations • 17ahydroxyprogesteronecaproate • Esterified derivative of 17a hydroxyprogesterone • Substantial progestational activity, long duration of action • Micronized progesterone in a gel • Micronized progesterone suppositories
Trials of Progestogens • Results of several small trials in the 1960’s and 1970’s suggested progesterone therapy may be effective in preventing preterm birth • Not all trials showed positive results • Meta-analyses produced conflicting results • The most successful trials employed 17-a Hydroxyprogesterone Caproate, (17P)
Meta-analysis of 17P in pregnancy • 5 trials: high risk women with 17P • Pooled analysis of results showed: • Reduction in rates of preterm birth Odds ratio 0.50, 95% CI: 0.30-0.85 • Reduction in rates of low birthweight Odds ratio 0.46, 95% CI: 0.27-0.80 Keirse MJNC. Brit J Obstet Gynecol 1990;97:149
Prior preterm birth Multifetal gestation Preterm birth Progestins & Prematurity Prevention Short cervix
Prophylactic administration of progesterone by vaginal suppository to reduce the incidence of spontaneous preterm birth in women at increased risk: A randomized placebo-controlled double-blind study • University of Sao Paulo Medical School, Brazil • RCT double-blind, placebo controlled • 1996-2001 • Rx: daily Progesterone (100 mg) vs placebo as vaginal suppository from 24 – 34 wks Da Fonseca et al AJOG 2003;188:419-24
Methods • 157 high risk singleton pregnancies, 15(9.5%) lost to follow-up; • Prior sPTD (avg 33 wks) • Prophylactic cervical cerclage • Uterine malformation • Analyzed remaining 142 • 70 placebo • 72 progesterone Da Fonseca et al AJOG 2003;188:419-24
Characteristics Prog Placebo • Qualifying delivery (wks) 33.3 33.4 • Maternal age (yrs) 27.6 26.8 • Caucasian 68% 71% • Risk Factor • Prior PTD 90% 97% • Uterine malformation 5.6% 1.4% • Incompetent cervix 4.1% 1.4% Da Fonseca et al AJOG 2003;188:419-24
Rates of Preterm Birth Placebo Placebo Prog Placebo Prog Prog P<0.002 P<0.03 NS Da Fonseca et al AJOG 2003;188:419-24
Uterine contraction frequency1 hr monitoring/wk Placebo Progesterone UC/hr P<0.004 Gestational age (wk) Da Fonseca et al AJOG 2003;188:419-24
NICHD: MFMU Progesterone Trial • Aim: To establish if weekly progesterone injections in women with prior spontaneous preterm delivery (sPTD) reduces the risk of PTD • Design: double-masked, placebo-controlled trial • Eligibility criteria: singleton pregnancy 16-20 wks with documented previous sPTD • Intervention: progesterone or placebo • 1o outcome: delivery <37 wks • Sample: 463 pregnant women Meis et al, N Engl J Med 2003
19 Centers enrolled women with: • Documented history of spontaneous preterm birth at 200 to 366 weeks’ gestation in a previous pregnancy • Gestational age at entry of 15-203 weeks confirmed by ultrasound • Singleton gestation, with no major fetal anomalies Meis et al, N Engl J Med 2003
Characteristics 17-P Placebo • Qualifying delivery (wks) 30.5 31.3 • Maternal age (yrs) 26.0 26.5 • Married 51% 46% • African American 59% 58% • Mean BMI 26.9 25.9 • Smoking 22% 19%
Progesterone: Rates of Preterm Birth 17P 17P 17P 17P 17P African American Non African American P<0.0001 P<0.016 P<0.018 P=0.010 P=0.004 Meis et al, N Engl J Med 2003 Meis et al, N Engl J Med 2003
Progesterone prevents neonatal complications Placebo 17 P Placebo Placebo Placebo 17 P Placebo 17 P 17 P Meis et al, N Engl J Med 2003 Meis et al, N Engl J Med 2003
Compliance and Side Effects • Compliance with the weekly injections was excellent • 91.5% of the women received their injections at the scheduled time • Side effects were minor and were similar in the 17P and placebo groups
Effectiveness of Progesterone • 5-6 women with a previous sPTB would need to be treated to prevent one birth <37 wks • 12 women with a previous sPTB birth would need to be treated to prevent one birth <32 wks Low dose ASA to prevent CVA, NNT=102 B-blocker use in MI patients to prevent cardiac death NNT=42 Meis et al, N Engl J Med 2003 Meis et al, N Engl J Med 2003
Progesterone prevents recurrent preterm delivery • Weekly injections of progesterone prevented recurrent preterm birth and improved the neonatal outcome for pregnancies at risk • Effective in preventing very early as well as later preterm birth • Effective in both African American and Non-African American women Meis et al, N Engl J Med 2003 Meis et al, N Engl J Med 2003
Impact of progesterone to prevent recurrent preterm birth • 10,000 preterm births could have been prevented in 2002 if all eligible pregnant women at high risk for PTD received 17P • Resulting in reduction of preterm birth of ~2% Petrini et al, Obstet Gynecol 2005; 105(2)
Progesterone gel and PTD • 659 women with prior sPTB • GA 18-22.9 wks, randomized • Progesterone vaginal gel or placebo • 90mg natural progesterone (Replens) • Primary outcome: PTB<32 wks O’Brien et al, Ultrasound Obstet Gynecol 2007;30:687-96
Characteristics Prog Placebo • Maternal age (yrs) 27.1 27.3 • African American 25% 28% • Mean BMI 26.6 26.4 • Smoking 22% 19% • >1 Prior PTD 24% 26% • CL at randomization 3.7 3.7 O’Brien et al, Ultrasound Obstet Gynecol 2007;30:687-96
Vaginal progesterone gel and PTD % O’Brien et al, Ultrasound Obstet Gynecol 2007;30:687-96
Summary: Progesterone & recurrent PTD • progesterone suppository & 17aOHPC IM: Significant reductions in PTD • Progesterone gel: no effect on PTD progesterone PTD 17P 17P
Prior preterm birth Multifetal gestation Preterm birth Progestins & Prematurity Prevention Short cervix
STTARS Seventeen alpha-hydroxyprogesterone caproate in Twins and Triplets: A Randomized Study) • Double-masked placebo-controlled trial to determine whether 17 a hydroxyprogesterone prevents preterm birth in multifetal pregnancies. • Intervention: 17-OHPC (250mg IM) or placebo weekly beginning at 16-20 weeks • Primary outcome: Preterm delivery < 35 wks • 661 women randomized Rouse et al, NEJM 2007; 357:454-61
Progesterone and Twins Characteristics: Prog Placebo • Maternal age (yrs)30 30 • Caucasian 67% 65% • Ob history • Nulliparous 46% 43% • Prior PTD 6% 9% • BMI 26.7 27.1 Rouse et al, NEJM 2007; 357:454-61
Twins: Delivery or Fetal Death Prior to 37, 35, 32 or 28 weeks 17-OHPC Placebo Similar findings for triplets Rouse et al, NEJM 2007; 357:454-61
Delivery or Fetal Death Before 35 WeeksBy Conception Method & Chorionicity Similar findings for triplets Rouse et al, NEJM 2007; 357:454-61
STTARS Seventeen alpha-hydroxyprogesterone caproate in Twins and Triplets: A Randomized Study) • 17P did not reduce the rate of PTB in women with twins • This lack of benefit applied: - whether conception was spontaneous or after ART or - whether there was a di- or monochorionic placentation - regardless of gestational age cutoff • 17-OHPC was well tolerated with side effects limited to the injection site • The rate of PTB in the placebo group was similar to national norms (34.9 vs 35.2 weeks) Rouse et al, NEJM 2007; 357:454-61
Prior preterm birth Multifetal gestation Preterm birth Progestins & Prematurity Prevention Short cervix
Cervical length Normal cervical length Short cervix with funneling
Cervical length at 24 wks predicts PTB risk Relative risk of sPTD <35wks by % of cervical length at 24 wks Iams et al, NEJM 1996
Considerations • Study population heterogeneity • Other risk factors for PTB • multiple gestation • prior preterm birth • Gestational age assessment of cervical length • Cervical length varies across gestational age • Cut-off selected depends on time of screening
Cervical length assessment Fonseca 20-25 <37 weeks <15mm (1.7%) N=24,620
Progesterone and short cervix: DeFrancosubanalysis of O’Brien trial: progesterone gel • 46 women with ≤ 28 mm cervical length • 19 progesterone (4 without PTB + 15 with PTB) • 27 placebo (5 without PTB + 22 with PTB) % “…these conclusions must be considered tentative...(and) hypothesis generating… (and)… further investigation is necessary. Specifically randomized clinical trials designed to test the effect of progesterone in women with a short cervix…” DeFranco et al, Ultrasound Obstet Gynecol 2007;30:697-705
Progesterone and short cervix: Fonseca trial: progesterone suppository • Cervical length 20-25 wks (24,620 women) • 413 CL <15mm (1.7%) • RCT: 250 women with cervical length ≤ 15mm • Progesterone 200 mg* PV daily vs. placebo • Micronized progesterone (Utrogestan, Besins International Belgium) • Initiation of treatment at 24 weeks *twice the dose of the daFonseca trial AJOG 2003 Fonseca et al, NEJM 2007; 357:462-9
Progesterone and short cervix: Fonseca trial: progesterone suppository Prog Placebo • Maternal age (yrs)29 29 • Caucasian 37% 39% • Ob history • Nulliparous 57% 55% • Prior PTD 12% 18% • Twin gestation 9% 10% Fonseca et al, NEJM 2007; 357:462-9
Progesterone and short cervix: Fonseca trial: progesterone suppository n=125 n=125 • Progesterone reduced risk of PTD in women with short cervix • No reduction in perinatal mortality or neonatal morbidity PTD<34 weeks Fonseca et al, NEJM 2007; 357:462-9
Progesterone and short cervix: Fonseca trial: progesterone suppository
Progesterone and short cervix: Fonseca trial: progesterone suppository • Very heterogeneous study group • Includes women with prior PTD, multiple gestations • Subgroup analysis of nulliparous women has OR that crosses unity
19 to 23 6/67 weeks Singleton Cervix 10-20 mm Nullips and multips (with prior term and preterm birth) Outcome: PTB < 33 weeks N = 465 Progesterone and short cervix: Hassan trial: progesterone gel Hassan et al, 2011 Ultrasound Obstet Gynecol
Progesterone and short cervix: Hassan trial: progesterone gel *P < .05 PTB% * * Hassan et al, 2011 Ultrasound Obstet Gynecol