Download
1 / 47
470 likes | 685 Vues
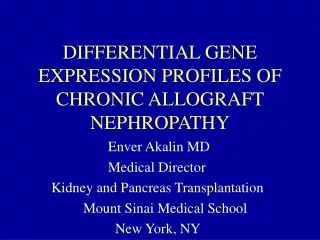
DIFFERENTIAL GENE EXPRESSION PROFILES OF CHRONIC ALLOGRAFT NEPHROPATHY. Enver Akalin MD Medical Director Kidney and Pancreas Transplantation Mount Sinai Medical School New York, NY. CHRONIC ALLOGRAFT NEPHROPATHY. Leading cause of allograft failure after patient death

E N D
DIFFERENTIAL GENE EXPRESSION PROFILES OF CHRONIC ALLOGRAFT NEPHROPATHY Enver Akalin MD Medical Director Kidney and Pancreas Transplantation Mount Sinai Medical School New York, NY
CHRONIC ALLOGRAFT NEPHROPATHY • Leading cause of allograft failure after patient death • Despite decrease in acute rejection rates, protocol biopsies still indicated ~ 50% CAN findings at 1 year protocol biopsies • Bohmig et al. Transplant Int 2005; 18: 131 • Current Banff CAN score is based on extent of fibrosis and does not provide information about cause, progression, or the treatment of allograft injury
Chronic Allograft Nephropathy: nodular arteriolar hyalinization (calcineurin inhibitor toxicity)
CHRONIC ALLOGRAFT NEPHROPATHY Non-immunologic factors Ischemia/reperfusion Delayed graft function Donor factors: Age Immunologic Factors Acute or subclinical rejection HLA mismatch Donor specific antibodies Calcineurin inhibitor toxicity Viral nephritis (Polyoma, CMV) Post-transplant HTN Hyperlipidemia Inflammation and injury Accelerated Senescence Adhesion molecules, cytokines and growth factors Interstitial fibrosis, tubular atrophy, transplant glomerulopathy, and fibrous intimal thickening of arteries
Chronic renal failure after transplantation of a nonrenal organ (69,321 persons who received transplantation in USA between 1990-2000)N Engl J Med 2003; 349:931
The natural history of chronic allograft nephropathy (Follow-up 119 kidney/pancreas transplant recipients by protocol biopsies up to 10 years)New Engl J Med 2003;349:2326
DONOR SPECIFIC ANTI-HLA ANTIBODIES • Anti-donor HLA antibodies are detected in 12-60% of recipients after transplantation • The sensitivity and specificity of detecting anti-HLA antibody is increased by utilizing ELISA or Flow Beads, as compared to CDC methods • Kidney transplant recipients with donor specific anti-HLA antibodies demonstrated 2-10 fold higher incidence of acute rejection and 5-6 times more likely developing chronic rejection • 5 year graft survival was 34% in patients with anti-HLA antibodies, compared to 76% without antibodies. • McKenna et al. Transplantation 2000; 69:319
ANTI-HLA ANTIBODIES • Prospective analyses of 139 patients for 8 years by yearly anti-HLA antibodies demonstrated that 29 patients developed chronic rejection and 100% of these patients had anti-HLA antibodies before rejection. 14 developed antibodies de novo. In contrast, 27% of 110 stable patients developed post-transplant anti-HLA antibodies. • Lee et al. Transplantation 2002; 74:1192 • In a prospective, multicenter study 2,278 patients F/U by anti-HLA antibodies for a year. 500 patients with anti-HLA antibodies had 6.6% graft failure in a year compared to 3.3% of 1,987 patients without anti-HLA antibodies. • Terasaki et al. Am J Transplant 2004; 4: 438
C4d • The presence of C4d in allograft biopsy samples is accepted as a finding of an acute or chronic humoral alloimmune response • 61% of biopsy samples with chronic transplant glomerulopathy/arteriopathy had positive C4d staining (12% of all CAN biopsies), and 88% of these patients had donor anti- HLA antibody • Mauiyyedi et al. J Am Soc Nephrol 2000; 12:574
C4d • 50% of CAN biopsies had + C4d staining and these patients demonstrated lower graft survival (4 vs 8 years of half life) • Lederer et al. Kidney Int 2001; 59: 334 • C4d deposits in PTC were detected in 73 of 213 late biopsies (34%) performed in 213 patients more than 12 mo after Tx (median, 4.9 yr) because of chronic allograft dysfunction. Endothelial C4d deposition was found to be associated with chronic transplant glomerulopathy and basement membrane multilayering • Regele et al. J Am Soc Nephrol 2002; 13: 2371
IMMUNE ACTIVATION IN CAN We investigated the role of chemokines (Mig, IP-10, and MCP-1) and chemokine receptors (CXCR3 and CCR2) and ICOS in chronic allograft nephropathy by immunohistopathologic examination of renal biopsy samples • Akalin et al. Am J Transplant 2003; 3:1116
Leukocyte labeling within glomeruli of renal biopsies from patients with CAN
Chronic Allograft Nephropathy plus Transplant Glomerulopathy
CONCLUSIONS • Increased expression of chemokines, their receptors, and ICOS on leukocytes in biopsies showing CAN and TGP vs. CAN alone suggest different underlying pathologic mechanisms • CXCR3-Mig/IP-10 pathway may play important role in the pathogenesis of TGP • Targeting chemokines or chemokine receptors and/or immune intervention may have clinical application in prevention and treatment of TGP
Diagnostic criteria's for chronic humoral rejection • Allograft histopathology (3/4 required) • Arterial intimal fibrosis • Duplication of glomerular basement membrane • Laminated PTC basement membrane • Interstitial fibrosis and/or tubular atrophy • C4d positivity at PTC • Serologic evidence of donor anti-HLA antibodies • Takemoto et al. Am J Transplant 2004; 4: 1033
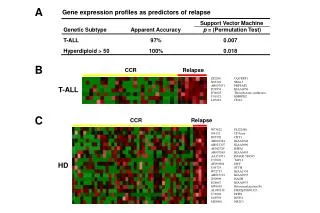
GENECHIP TECHNOLOGY • Has the power to measure the expression of thousands of human genes simultaneously. • Currently two types of methods, oligonucleotide and cDNA microarrays, have been successfully used to analyze the gene expression patterns of different types of cancers and inflammatory diseases for diagnosis, and to predict prognosis and response to therapy. • Hypothesis-generating, rather than hypothesis-driven
GENECHIP AND CHRONIC ALLOGRAFT NEPHROPATHY • Gene expression profiles of 17 protocol kidney biopsies at 6 months after transplantation were studied by oligonucleotide arrays to predict the development of CAN at 12 months • Patients were on RAD B251 study (Certican versus Cellcept with Neoral and prednisone) • 9 patients developed CAN at 12 months (All were on Certican) • 10 genes might predict the development of chronic rejection (8 upregulated, 2 downregulated) • Those genes were APRIL (acidic protein rich in leucins), OBCML (opiate-binding protein-cell adhesion molecule like), the tumor suppressor gene NPRL2, cytokeratin 15, homeobox gene B7, prolactin receptor, and guanine nucleotide binding protein gamma 7. • Scherer et al. Transplantation 2003; 75: 1323
GENECHIP ANALYSIS OF TRANSPLANT NEPHRECTOMIES • Gene expression patterns of 13 transplant nephrectomy samples with chronic rejection comparing to 16 normal kidneys (histologically normal part of tumor nephrectomy samples) and 12 PCKD nephrectomy samples were studied by using cDNA arrays • Hierarchical clustering analysis revealed two distinct subsets of chronic rejection • 22 genes were upregulated and 6 were downregulated in CAN biopsies compared to PCKD nephrectomy samples • Donauer et al. Transplantation 2003; 76: 539
GENECHIP AND KIDNEY TRANSPLANTATION • 67 allograft kidney biopsies from 50 pediatric patients were analyzed by cDNA arrays • While the gene expression patterns suggested at least 3 possible distinct subtypes of acute rejection, 19 CAN biopsy samples were clustered together without demonstrating any subset • Sarwal et al. N Engl J Med 2003; 349: 125
GENECHIP IN CALCINEURIN INHIBITOR AVOIDANCE STUDY • Patients were randomized into 2 groups: • CsA+MMF+Pred+Basiliximab • Rapa+MMF+Pred+Basiliximab • 61 patients were enrolled. • 55 patients underwent renal function studies and 48 patients had protocol biopsies at 2 years after transplantation • 41 were analyzed by Affymetrix GeneChip • Flechner et al. Am J Transplant 2004, 4:1776
GENECHIP IN CALCINEURIN INHIBITOR AVOIDANCE STUDY • Comparison of CsA/MMF/P group to SRL/MMP/P group yielded 379 differentially expressed genes and 97% of the genes are upregulated in the CsA-treated patient biopsies • Comparison of combined Banff 2 and 3 biopsies to Banff 0 biopsies in revealed significant upregulation of genes responsible for immune/inflammation and fibrous/tissue remodeling
Gene names Fold change by GeneChip GeneChip p-values2 Fold change by Q-PCR Q-PCR p-values4 Matrix metalloproteinase 7 (47) 3.22 0.000001 15.01 0.026 TIMP1 (48) 2.25 0.000003 3.02 0.0855 CCL5 (RANTES) (49) 1.55 0.0004 5.51 0.035 VEGF (50) 1.57 0.0008 5.62 0.040 Collagen III (51) 2.52 0.003 24.31 0.010 MCP1/CCL2 (52) 1.36 0.003 2.82 0.043 Fibronectin (38) 1.70 0.005 19.66 0.005 TNF alpha (53) 1.58 0.008 189.09 0.026 Angiotensin II receptor (54) 1.12 >0.013 12.80 0.006 TGF beta (55) 1.28 >0.013 2.17 0.1625 PDGF (56) 1.06 >0.013 2.32 0.1775 GENECHIP ANALYSIS OF PROTOCOL BIOPSIES AT 2 YEARS
STUDY AIMS • To characterize gene expression patterns in transplant kidneys with CAN by comparing them to the expression patterns of transplant kidneys with normal histopathology. • To correlate gene expression profiles in CAN with clinical features including positive donor specific antibodies, C4d staining, transplant glomerulopathy, and nodular arteriolar hyalinization
METHODS • One piece of allograft biopsy was snap frozen in liquid nitrogen at the time of a clinically indicated biopsy (rising creatinine and/or proteinuria). • Biopsies were evaluated according to the Banff criteria, and were further stained for C4d antibodies. • Donor specific antibodies were studied by Flow Beads (Luminex)
METHODS • High-density oligonucleotide arrays (Affymetrix HG-U133A contains 22,283 probe sets representing about 16,000 genes per chip) were used for gene expression analyses • Hierarchical cluster analysis was chosen as a cluster analysis technique • Statistical modeling included Robust Multi Array (RMA) to normalize the data and Significance Analysis of Microarray (SAM) to identify the most significant genes
B B B B B B B B B B B B Biotin - labeled cRNA transcript Cells AAAA IVT Biotin-UTP Biotin-CTP Poly (A)+ RNA cDNA Fragment heat, Mg2+ Add polyA Controls Hybridize (16 hours) Wash & Stain Scan (75 minutes) Add Oligo B2 & Staggered Spike Controls (8 minutes)
GENECHIP RESULTS • Among 22,283 probe sets, representing about 16,000 genes per chip, 37-59% of genes were present in all samples • Replicated samples demonstrated less than 0.03% gene expression difference with a high degree of correlation reflecting by R2 of 0.983 and 0.989
RESULTS • 455 probe sets representing 324 genes were differentially expressed in CAN biopsies compared to controls. While 212 genes were upregulated a minimum of 1.5 fold, 112 genes were downregulated in CAN samples. • Biological functions of differentially expressed genes: • Cellular metabolism: 171 (53%) • Cellular communication: 105 (32%) • Cell growth/maintenance: 103 (32%) • Signal transduction: 79 (24%) • Cell adhesion: 39 (9%) • Immune response: 31 (9%) • Apoptosis: 12 (4%) • Blood coagulation: 12 (4%) • Humoral defense mechanism: 5 (2%) • Complement: 5 (2%) • Function unknown: 24 (7%)
RESULTS • Selected upregulated genes related to immunology • Transforming growth factor-β induced factor and thrombospondin-1, which played role in TGF- signaling pathway, and platelet derived growth factor-C • The chemokine CXCL-6, and the adhesion molecules vascular cell adhesion molecule, cell adhesion molecule with homology to L1CAM, activated leukocyte cell adhesion molecule and selectin P • The complement-related upregulated genes were complement component 4A and 4B, I factor, B factor (properdin), and clusterin (complement lysis inhibitor) • The other upregulated immune response related genes were; MHC class II DR 4, and DP1, interferon- inducible protein, interferon induced protein 44, IL-17B receptor, natural killer cell transcript 4, CD24, and CD59.
RESULTS • Other selected genes: • Genes related to fibrosis and extracellular matrix deposition, such as; versican (chondroitin sulfate proteoglycan 2), integrin-beta 3 and 6, matrix metalloproteinase 7, 9 and 10, laminin, fibronectin, tenascin, glypican 3 and 4, collagen type IV alpha 2, disintegrin, and cadherin 2 and 6 • claudin 3, annexin A1, A3 and A4, connexin, which are related to tight junction between cells
RESULTS • Selected downregulated genes: • Significant number of downregulated genes were podocyte related, such as; podocin, nephrin, Wilms tumor 1, podocalyxin, and synaptopodin, or renal-specific genes; renin, calbindin, adrenomedullin, stanniocalcin, and kininogen • vascular endothelial growth factor, epidermal growth factor, and fibroblast growth factors 1 and 9, insulin-like growth factor binding protein 3 and 5
RESULTS • In one sample with both strong C4d staining and positive DSA, more than 50% of the 100 genes with the highest hybridization intensities in comparison analyses were related to: • immunoglobulin structures, • complement (C3, C4a, C4b, C1q, complement factor H and I), • B cells (CD20 and CD48), • T cell receptor, nuclear factor of activated T cells, natural killer cell, • cytokine receptors (Interleukin-2, 7, and 10 receptor), • chemokines (Humig, MCP 1, RANTES), chemokine receptors (CCR2 and CCR7)
VASCULAR ENDOTHELIAL GROWTH FACTOR • VEGF regulates angiogenesis, vascular permeability, endothelial cell migration and proliferation. • VEGF plays role in the maintenance and formation of podocytes and establishes glomerular filtration barrier • VEGF-A knockout mice (homozygous) die at birth with hydrops and renal failure and podocyte specific heterozygosity of VEGF-A resulted in proteinuria and endotheliosis at 2.5 weeks of age resembling preeclampsia • Eremina et al. J Clin Invest 2003; 111: 707
VEGF FOR CYTOPROTECTION • VEGF levels are decreased in preeklampsia • VEGF is protective against cyclosporin nephrotoxicity • Caramelo et al. Nephrol Dial Transpl 2004; 19: 285 • VEGF and fibroblast factor-1 was downregulated in biopsies with diabetic nephropathy by genechip and immunohistopathology • Am J Kidney Dis 2004; 43: 636
VEGF FOR PROINFLAMMATION • VEGF is upregulated in mice models of acute and chronic rejection • VEGF is upregulated in human heart and kidney biopsies with chronic rejection • Reinders et al. Transplantation 2003; 76: 224 • Pilmore et al. Transplantation 1999; 67: 929 • VEGF is upregulated in experimental models of diabetic nephropathy
CONCLUSIONS • A number of genes are differentially expressed in biopsies with CAN compared to normal transplant kidney biopsies by GeneChip technology. • Some of the upregulated genes are related to fibrosis (MMP-7, 9, and 10, laminin, fibronectin, and tenascin) or factors/cytokines, which induce fibrosis (TGF-β, thrombospondin-1, and PDGF). • Gene expression of VEGF, EGF, FGF-1 and 9 were downregulated in CAN. Immunpathologic examination indicated the lack of VEGF production by the glomerular cells in CAN. • Hierarchical cluster analyses demonstrated that CAN samples did not show distinct subsets, including biopsies with nodular hyalinosis. • Gene expression profile of one patient withpositive C4d staining and donor-specific anti-HLA antibodies indicated the role of immune-mediated mechanisms.
ROUTINE C4d STAINING • Since July 2003, all clinically indicated transplant kidney biopsies were routinely studied by C4d staining and patients with positive C4d staining were routinely studied for donor-specific anti-HLA antibodies (DSAs) by Flow Beads (Luminex) • 166 biopsies from 128 patients demonstrated that 22 biopsies (13%) from 11 patients (9%) were C4d + • 9 patients with C4d+ had early AHR and 2 had CAN • All C4d+ patients had DSAs • Only 2 out of 62 biopsies (3%) with CAN (22 grade I, 26 grade II, and 14 grade III) were C4d + • There were 11 CAN biopsies with transplant glomerulopathy, and 4 with secondary focal segmental glomerulosclerosis, and all were C4d negative
ROUTINE C4d STAINING • 54 biopsies in 43 patients showed CAN • 20 biopsies (37%) exhibited transplant glomerulopathy and none showed peritubular C4d staining • Only 2 biopsies were C4d +. One had DSAs and the other had no detectable DSAs • Aly et al. Transplant Int 2005; 18: 800
LIMITATIONS OF MICROARRAY STUDIES IN CAN • GeneChip technology has been used in CAN patients in a limited number of studies involving limited number of patients (< 20) • Difficulty in evaluating vast quantities of data to reach a meaningful conclusion in a limited number of heterogeneous group of patients and immunosuppressive medications for a very heterogeneous disease like CAN • Tissue sampling differences, as biopsy samples contain a mixture of different cell and tissue types, involving varying proportions of muscle, capsule, cortex and medulla of the kidney • Limited amount of total RNA • The data analysis of microarrays is still in its infancy and there is no universally accepted method
FUTURE DIRECTIONS • In order for microarray studies to define certain subgroups of patients for diagnosis, prognosis, and management of CAN, or find candidate genes, novel pathways, and/or surrogate markers, hundreds of biopsies should be performed in multicenter collaborative studies with a prospective manner starting microarray analysis of transplant kidney biopsies before implantation and follow-up protocol biopsies until CAN develops • Microdissected samples should be used to avoid sampling errors