Download
1 / 11
110 likes | 292 Vues
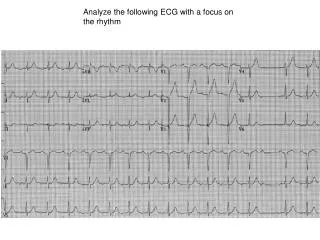
Analyze the following ECG with a focus on the rhythm. 1-What is the baseline rhythm?. P is (-) in I, (+) in aVR -this could mean the rhythm is not a sinus rhythm, i.e., ectopic atrial rhythm OR -it c ould be arm electrode reversal

E N D
1-What is the baseline rhythm? • P is (-) in I, (+) in aVR • -this could mean the rhythm is not a sinus rhythm, i.e., ectopic atrial rhythm OR -it could be arm electrode reversal • In case of arm lead reversal: P, QRS, and T will be inverted in I and aVL, not just P wave. The P/QRS/T in lead I will be flipped over, while the complexes in leads aVL and aVR are switched this is not the case here, thus it is an ectopic atrial rhythm
2-How do you explain the pause? • A pause has 3 causes: 1-Sinus pause: in this case, no blocked P is seen within the pause (the sinus node is “sleeping”, thus no P or QRS are seen) 2-AV block (2nd degree): a blocked P is seen within the pause. The blocked P marches out with the regularly occuring baseline P 3-Blocked PAC: : a blocked P is seen within the pause, sometimes over the preceding ST/T. The blocked P does not march out with the regularly occuring baseline P and actually comes prematurely
Which ones of these 3 causes of pause are benign? • Blocked PAC is the most benign of the 3 diagnoses • Sinus pause, if short < 3sec or esp. if asymptomatic, is benign • AV block is benign if it is 2nd degree Mobitz 1. It is ominous if it is 2nd degree Mobitz 2, even if it is just an asymptomatic brief pause
In our case, there is a blcked P within the pause that marches out with the preceding P wavesThis is AV block (see next Figure)
P P P P Blocked P marches out with preceding P waves
3-Is it a Mobitz 1 or Mobitz 2 second-degree AV block? • In Mobitz 1, PR progressively prolongs before the pause, while in Mobitz 2, there is a sudden block of P conduction without any preceding PR prolongation • However, in case of a very slowly progressive PR prolongation, it may seem that PR is not prolonging, and Mobitz 1 may be misdiagnosed as Mobitz 2. That is why it is best to look at the PR just preceding the block and compare it to the PR that follows the block
Ectopic P Ectopic P See how PR that precedes the block is longer than PR that comes after the block- Mobitz 1 Final ECG dx: Ectopic atrial rhythm rate of 95 bpm with Mobitz 1 (Wenckebach) AV block
P drops without progressive PR prolongation=Mobitz 2. Rate~60 and the pt is asymptomatic, it would seem innocuous but this is actually ominous because it is Mobitz 2. Mobitz 1 is benign. That is why it so important to carefully analyze every small pause. A benign Mobitz 1 or a blocked PAC may very well simulate the malignant Mobitz 2
Location of AV block Mobitz 1 is usually a nodal blockthe QRS is often narrow. Mobitz 1 rarely progresses to complete AV block and is often asymptomatic Mobitz 2 is an infranodal blockthe QRS is often wide. Mobitz 2 is ominous even if asymptomatic, it can progress to a bad complete AV block with slow ventricular escape
Am example of 2: 1 AV block In 2:1 AV block, there is only one conducted QRS before the dropped QRS, thus you cannot tell if the dropped QRS is preceded by progressive PR prolongation or not, i.e. Mobitz 1 or 2. In order to say Mobitz 1 or 2 in case of 2:1 AV block, rely on the width of QRS. If QRS is wide, it is an infranodal block, i.e. Mobitz 2, ominous; if QRS is narrow, it is Mobitz 1. The 2:1 AV block on the current ECG is therefore Mobitz 2 AV block.