Download
1 / 24
240 likes | 363 Vues
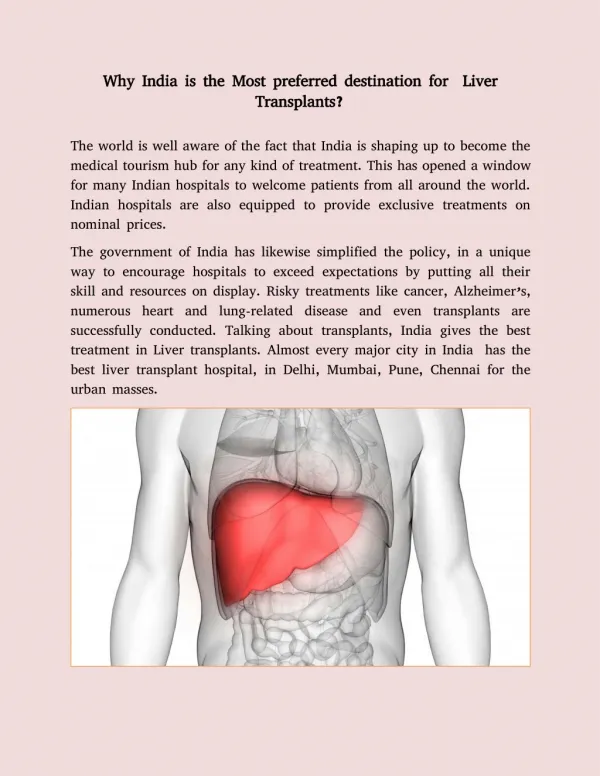
Liver Transplants for PLWHA in Spain 10 years of activism. Xavier Franquet xfranquet@gtt-vih.org Grupo de Trabajo sobre Tratamientos del VIH (gTt) Foro Español de Activistas en Tratamientos del VIH (FEAT). Spain: A Large Scale Epidemic in Southern Europe. Total population: 45 million

E N D
Liver Transplants for PLWHA in Spain10 years of activism Xavier Franquet xfranquet@gtt-vih.org Grupo de Trabajo sobre Tratamientos del VIH (gTt) Foro Español de Activistas en Tratamientos del VIH (FEAT)
Spain: A Large Scale Epidemic in Southern Europe • Total population: 45 million • UNAIDS estimation: 120,000-150,000 PLWHA • HCV / HIV Co-infected (45-50%) 60,000-80,000 • HBV / HIV Co-infected ( 5-7% ) 5,000-10,000
When Hepatitis Treatment Doesn’t Work • HCV genotype 1 is difficult to treat and predominant in Spain. • HCV treatment works worse in co-infected with HIV. • HCV liver damage progresses faster in co-infected. More than 7,000 PLWHA with liver cirrhosis in Spain. More than 2,000 need a liver transplant urgently.
1998 • PLWHA were excluded from liver transplants. • Fear that transplant related immunosuppression could speed up the progression to AIDS or increase the risk of opportunistic infections. • HAART was introduced in 1996. • HIV could now be controlled. • Liver damage by viral hepatitis was progressing rapidly.
1998 Jordi Riba, a doctor living with HIV and end stage liver disease founded an activist group: ATOS (Association for Organ Transplants for PLWHA) was the first community group to raise the issue. Objectives: • Review the absolute exclusion criteria and remove it. • Promote a study to assess the survival rates of PLWHA after organ transplants.
Barcelona, 1998Demonstrations in front of the regional government building
Barcelona, 1998 Civil society reaction Public personalities supporting the cause
1998 • Jordi Riba died. • June 1998: The Spanish Minister of Health meets the Local Catalan Health Authorities (Barcelona). • Most HIV doctors were in favor. • Most hepatologists and transplant surgeons against.
Making a study protocol • Liver Transplant Units, hepatologists and HIV doctors in Catalonia were leading the process. • Feb 1999. First draft of a study protocol. • 2001. Protocol is completed. • 2001. Spanish Transplant Units stepped down leaving Catalan hospitals on their own.
2002 : First Liver Transplant in HIV+ in Spain • 4th August, 2002. Hospital de Bellvitge (Barcelona) • HIV community groups were very active. Working together with HIV doctors, trying to make transplant units change their mind. • Gradually other hospitals in Spain gave access to liver transplants for HIV+.
2004: More than 2,000 PLWHA in need of an urgent liver transplant in Spain
2004: Spanish Consensus Document • May 2004, Bilbao. 11th Congress of the Spanish InfectiousDisease and Clinical Microbiology Society. • Presentation of the first 26 liver transplants in Spain • 81% Co-infected with HCV • 11% Co-infected with HBV • 8% Co-infected with HCV and HBV • Similar survival rate as that observed in HIV negative patients
2004: Spanish Consensus Document • AIDS Study Group (GESIDA) of the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC). • Infection in Transplant Study Group (GESITRA). • Liver Unit. Hospital Clínic. Barcelona. • Digestive Surgery Service. Hospital de Bellvitge. Hospitalet de Llobregat Barcelona. • Action Guidelines Committee for Viral Diseases in Haemodialysis of the Spanish Nephrology Society. • Transplant and Cardiac Insufficiency Study Group of theSpanish Heart Society. • Programme for the Prevention and Care of AIDS in Catalonia. • Catalonian Transplant Organization (OCATT). • Government Delegation for the National Drugs Plan, Ministry of Health (MSC). • National AIDS Plan Secretariat (PNS) of the MSC. • National Transplant Organization of the MSC.
2004: Spanish Consensus Document 12) State Coordinator of Associations for the Fight against AIDS (CESIDA) 13) The Spanish HIV Treatment Activists Forum (FEAT) Published in 2005 : Enferm Infecc Microbiol Clin 2005;23(6):353-62
2005: Spanish Consensus DocumentSpecific criteria for PLWHA • No opportunistic infections, except: tuberculosis, oesophageal candidiasis, P. Jiroveci pneumonia. • CD4 lymphocyte count above 100 cells/mm3 for liver transplant (above 200 cells if any OI from above in the past). • Undetectable viral load or suppressible with antirretroviral therapy. • 2 year abstinence from heroin and cocaine (being in a methadone program permitted) and 6 months abstinence from alcohol and other drugs. • Favorable report after mental health and social assessment.
Specific criteria for PLWHAAllegations from the HIV Community • No opportunistic infections, except: tuberculosis, oesophageal candidiasis, P. Jiroveci pneumonia. • CD4 lymphocyte count above 100 cells/mm3 for liver transplant (above 200 cells if any OI from above in the past). These are very restrictive criteria! • Other OI in the past should be allowed • Previous data in transplant recipients shows the risk for OI increases below 100 CD4 and not between 100-200 CD4.
Specific criteria for PLWHAAllegations from the HIV Community • 2 year abstinence from heroin and cocaine (being in a methadone program permitted) and 6 months abstinence from alcohol and other drugs. These are very arbitrary requirements! • Find good psychiatrist/toxicologist advice. • No different times for different drugs: 6 months abstinence for all (no exclusion of cannabis). • Allow patients in heroin maintenance programs.
Specific criteria for PLWHAAllegations from the HIV Community • Favorable report after mental health and social assessment. We identified prejudices about previous drug use! • Participation of HIV community representatives in the multidisciplinary teams
Liver Transplant for PLWHA: The Challenges Pre-Transplant • Fast progression of liver damage in co-infected patients. • High rates of exclusion from the waiting list following current criteria (higher than 50%). • High mortality rates in waiting lists (higher than 50%).
Liver Transplant for PLWHA: The Challenges Post-Transplant • Graft rejection. • Management of relapse of HCV infection (HCV re-infection is considered universal). Need of: • Better donor selection. • More efficient HCV treatment. • Pharmacokinetic and pharmacodynamic interactions between ARV and immunosuppressors (specially boosted PI).
Liver Transplant for PLWHA: The HIV Community Concerns • Too restrictive inclusion criteria for PLWHA. • New consensus document in 2009 • Geographical differences in access. • PLWHA enter the waiting list too late (fast liver cirrhosis progression) • Need for an early referral from HIV doctors to hepatologists and transplants units. • Need for assessment after first decompensation. • Limitation of the procedure. Not enough donors.
Esther Inés (Valencia, Spain) “The process of getting onto the waiting list for a liver transplant needs to be carried out with plenty of time, before you start feeling unwell. I do not recommend waiting until the last minute.” “We, as patients, need to be active, asking about the real chances we have of getting a liver transplant and motivating our HIV doctors to get in contact with the hepatologists as early as possible.” “We need to lead this process ourselves while we’re still mentally and clinically well”. “I wish you all a good conference”.
2008: Spanish Solid Organ Transplant HIV Cohort 140 transplants in 6 years • Most of them liver transplants • Majority in HCV / HIV Co-infected patients • After 6 years, same mortality rate as HIV negative patients. (67% at 4 years, analysis of the first 89 cases 2002-2006 presented at CROI, 2008)
Acknowledgements Juanse Hernández and my colleagues at Grupo de Trabajo sobre Tratamientos del VIH (gTt) (Barcelona) Foro Español de Activistas en Tratamientos del VIH (FEAT), especially to Esther Inés (Valencia), Udiarraga García (Bilbao) and Diego García (Alicante). Ferran Pujol and Michael Meulbroek, ATOS / HISPANOSIDA /CACSIDA Ramón Espacio, CALSICOVACA, CACSIDA Dr. Josep M. Miró, Hospital Clinic (Barcelona) and all the Spanish doctors, healthcare professionals and health authorities who always believed that we have the right to be candidates for transplants. This presentation is dedicated to all those waiting for a transplant.