Download
1 / 81
870 likes | 1.15k Vues
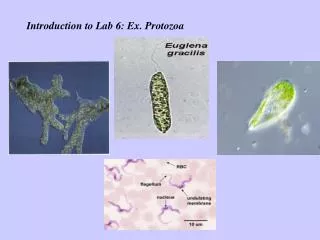
Blood & Tissue Protozoa Lange Chapter 52 Faculty: AGUAZIM SAMUEL, M.D. The medically important organisms:. The sporozoans: Plasmodium and Toxoplasma The flagellates: Trypanosoma and Leishmania. CASE.

E N D
Blood & Tissue Protozoa Lange Chapter 52 Faculty: AGUAZIM SAMUEL, M.D.
The medically important organisms: • The sporozoans:Plasmodium and Toxoplasma • The flagellates:Trypanosoma and Leishmania
CASE 40 year old male on a business trip to WEST AFRICA presented with sudden fever, joints pains and headache which were most severe every 3rd day. In between, he would fell weak, but the fever would lyse. He had vaccine for yellow fever and HAVRIX prior to leaving the US. He was staying in a urban hotel, and had limited trips except for the office.
CASE Thick blood smear showed:
CASE Impression: Malaria, probably non-Chloroquine resistant; secondary to Plasmodium species
PLASMODIUM • Disease:Malaria • Malaria is caused by four plasmodia:vivax, ovale, malariae, and falciparum. • Vivax and falciparumare more common causes of malaria than are ovale and malariae.
Malaria • 300–500 million infections worldwide and approximately 1 million deaths annually. • 10 million new cases • more than 2 million die of it each year, making it the most common lethal infectious disease. • http://www.cdc.gov/travel/other/malaria_dr_2004.htm
Important Properties of Malaria • The vector and definitive host for plasmodia is the femaleAnopheles mosquito (only the female takes a blood meal). There are two phases in the life cycle: • Sexual cycle, which occurs primarily in mosquitoes. • Asexual cycle, which occurs in humans the intermediate hosts.
13. Fertilization 14. Invasion of gut mucosa 15. Oocyte 16. Sporozoite 17. Released into gut 18. Salavary glands 1. Sporozoite 2. Parenchymal cells of the liver. 4. Mature in two weeks into schizonts. 5. Rupture to produce 10-40,000 merozoites. 6. Circulate for a few minutes before entering the red blood cell. 7. Merozoites mature into the ring form in the RBC. 8. From ring form to Trophozoite. 9. From Trophozoite to Schizont. 10. Completion of life cycle to release merozoites into the blood stream. 11. Some merozoites initiate the sexual stage to form male and female gametocytes. 12. Gametocytes taken up by the Anophles mosquito; eight male microgametes and female macrogametes are produced in the gut. Sexual Asexual
Pathogenesis of Malaria: • Most of the pathologic findings of malaria result from the destruction of red blood cells. • Red cells are destroyed both by the release of themerozoites and by the action of the spleen. • Malaria caused byP falciparumis more severe than that caused by other plasmodia. • It is characterized by infection of far more red cells than the other malarial species.
Malaria Clinical Findings • Abrupt onset offever, chills and Headache • Myalgias, about 2 weeks after the mosquito bite. • Fever may be continuous early in the disease • Untreated malaria caused byP. falciparumis potentially life-threatening as a result of extensive brain and kidney damage. • Malaria caused by the other three plasmodia is usually self-limited, with a low mortality rate. • life-threatening hemorrhage and necrosis,particularly in the brain(cerebral malaria). • Extensive hemolysis and kidney damage occur, with resultinghemoglobinuria. • The dark color of the patient’s urine has given rise to the term“blackwater fever.”
Malaria Clinical Differences between species: • P. falciparumcauses a high level of parasitemia, because it can infect red cells of all ages. • P vivaxinfects only reticulocytes. • P malariaeinfects only mature red cells; they produce much lower levels of parasites in the blood.
Sickle Cell Anemia and Malaria • Individuals withsickle cell traitare protected against malaria • Their red cells have too littleATPase activityand cannot produce sufficient energy to support the growth of the parasite.
Malaria and the Duffy antigen • The receptor forP vivaxis theDuffy blood • group antigen. • People who are homozygous recessive for the genes that encode this protein are resistant to infection byP. vivax. • More than 90% of blackWest Africansand many of their American descendants do notproduce theDuffyantigen. Homozygous: having identical genes at one or more loci
Malaria is transmitted primarily bymosquitobites, but transmission can occur: • across theplacenta • in bloodtransfusions • intravenous drug abusealso occur.
Laboratory Diagnosis of Malaria: • Diagnosis rests on microscopic examination ofblood, using boththick and thin Giemsa-stainedsmears. • - thick smear: used to screen for the presence of organisms • - thin smear is used for species identification.
It is important to identify the species, because the treatment of different species can differ. • Ring shaped trophozoitescan be seen within infected red blood cells. • The gametocytes ofP.falciparumarecrescent shaped (banana-shaped) • The gametocytes of the other plasmodia arespherical.
Treatment of Malaria: • http://www.artemisininproject.org/Current_Treatments • Chloroquine:acute malaria: (kills themerozoites)reducing the parasitemia. Check CDC for Chloroquine resistant areas!!! • Dose, 500 mg. orally per week for one week prior to travel, during travel and 4 week afterwards. • Chloroquine prophylaxis only effective for travelers to malaria-risk areas in: • - Mexico -Central America • - Haiti -Middle East • - Dominican Republic -Eastern Europe
Other Malaria Treatments • Forchloroquine resistantstrains of P falciparum:mefloquine, doxycyclineor a combination ofquinine and Fansidaris used. Neurologic side effects such as psychosis for Mefloquine. • Primaquine or Pyrimethamine: is used to treat thehypnozoites of P vivax and P ovalein the liver. Primaquine must be used to prevent relapses. • Malarone: new drug: combination of atovaquone and proguanil. First dose 1-3 days before travel, during travel and 7 days after travel. Can’t use in pregnant women, breast-feeding women and infants< 24 lbs.
Prevention of Malaria:Chemoprophylaxis • Travelers to areas where the plasmodia are found should take chloroquine starting 1-2 weeks before arrival and continuing for 4-6 weeks after departure. • Travelers to areas where chloroquine resistant P falciparumis endemic consists ofmefloquine.This should be followed by a 2-week course ofprimaquineif exposure was high. • use of mosquito netting, window screens, protective clothing, and insect repellents. • The mosquitoes feed from dusk to dawn, so protection is particularly important during the night.
Babesia Babesiosis: fever and hemolytic anemia(malaria-like) Predominantly in the northeastern U.S. Co-infection with borrelia Blood smear, no RBC pigment Appears as a “Maltese cross”(tetrad in RBCs) MOT: TICK BITE(ixodes tick) hemolytic anemia, jaundice, fever and hepatomegaly, usually 1-2 weeks after infection DOC: Clindamycin and quinine
Acanthamoeba castellanii Naegleria fowleri(FREE-LIVING AMEBA) "the brain-eating amoeba“ Rapidly fatal meningoencephalitis Swimming in freshwater lakes Their life cycle involves trophozoite and cyst stages. Cysts are quite resistant and are not killed by chlorination Enters via the cribriform plate Amoebas in spinal fluid AMP B MAY EFFECTIVE FOR NAEGLERIA Pentamidine, ketoconazole, or flucytosine may be effective in Acanthamoeba infections ACANTHAMOEBA ALSO CAUSES KERATITIS .
Toxoplasma gondii Disease: Toxoplasmosis
Toxoplasma Characteristics: • Tissue protozoan. • Life cycle in human: • Cysts in cat feces or meat • Ingested by humans • Differentiate in the gut and invade • Infectmacrophages • Formtrophozoites (tachyzoites)that multiply, kill cells, and infect other cells • Cystscontainingbradyzoitesform later in the host cell, brain, muscle, and other tissues!!!!!!
Infective form: oocysts Pathogenic form: tachyzoite
Toxoplasma Life cycle in cat: • 1. Cat ingests cysts in raw meat • 2.Bradyzoitesreleased from the cyst in the small intestine. • 3. Multiply, and form gametocytes. • 4. These fuse to formoocystsin cat gut, which are excreted in cat feces.
Toxoplasma Human infection:usually occurs from eating undercooked meat lamb or pork, from animals that grazed in soil contaminated with infected cat feces. Transmission: Transmitted by ingestion of cysts andtransplacentallyfrom mother to fetus. Cat is definitive host; humans and other mammals are intermediate hosts. Occurs worldwide.
CONGENITAL TOXOPLASMOSIS • classic clinical triad retinochoroiditis cerebral calcifications convulsion • TORCH • T – Toxoplasmosis • O – Others (VSZ and Parvovirus B19 • R – Rubella • C – CMV • HE – Herpes, HIV • S – Syphilis
Toxoplasma Pathogenesis: Trophozoites infect many organs, especially brain, eyes, and liver. Cysts persist in tissue. Laboratory Diagnosis:Serologic tests for IgM and IgG antibodies are usually used. Treatment:Sulfonamide and pyrimethamine for congenital or disseminated disease. Prevention:Meat should be cooked. Pregnant women should not handle cats, cat litter boxes, or raw meat.
Ring Enhancing lesion Toxoplasmosis
Trypanosoma cruzi (American Trypansomiasis) Disease:Chagas’ disease (American trypanosomiasis) Characteristics:Blood and tissue protozoan. Life cycle: 1. Trypomastigotes in blood of reservoir host 2. Ingested byreduviid bug ( kissing bug or cone bug) 3. Form epimastigotes 4. Formtrypomastigotesin the gut.
Riduvid bug, the vector of American trypanosomiasis cone-nose or kissing bug
Trypanosoma cruzi • When the bug bites, it defecates and feces containingtrypomastigotescontaminate the wound. • Organisms enter the blood and formamastigoteswithin cells; these then becometrypomastigotes. • Transmission: Transmitted by reduviid bugs. Humans and many animals are reservoirs. Occurs in rural Latin America. • Pathogenesis: Amastigotes kill cells, especially cardiac muscle
Trypanosoma cruzi • Laboratory Diagnosis: • Trypomastigotes visible in blood • But bone marrow biopsy, culture in vitro, or serologic tests may be required. Clinical findings: • facial edema (Ramana’s sign) • nodule (chagoma) near the the bite. • Complications include megacolon and enlarged heart. • DEATH FROM CHRONIC CHAGAS DZ IS USUALLY DUE TO CARDIAC ARRHYTHMIAS AND FAILURE
Trypanosoma cruzi, trypomastigote form, in a blood smear (Giemsa stain)CDC
Chagoma: raised, non-purulent erythematous plaque surrounded by hard edema
Trypanosoma cruzi Treatment:Nifurtimox for acute disease. No effective drug for chronic disease. Prevention:Protection from bite. Insect control.
Trypanosoma • Disease: Sleeping sickness (African trypanosomiasis) • Trypanosomiasis is a systemic disease caused by the parasite Trypanosoma brucei. • East African trypanosomiasis: T. rhodesiense • West African trypanosomiasis: T. gambiense. • It is transmitted by the bite of the tsetse fly, a gray-brown insect about the size of a honeybee.
Trypanosoma (African Sleeping Sickness) • Characteristics: Blood and tissue protozoan. • Life cycle: • Trypomastigotesin blood of human or animal reservoir, are ingested bytsetse fly. • 3. They differentiate in the gut to formepimastigotes • 4. Metacyclic trypomastigotesformed in salivary glands. • 5. When fly bites, trypomastigotes enter the blood. • 6. Repeated variation of surface antigen occurs, which allows the organism to evade the immune response. Recurrent Fever.