The Esophagus
The Esophagus. Historical Aspects. The earliest esophageal procedures were limited to the cervical region (removal of foreign bodies-1863) Modified ureteroscope used to diagnose carcinoma of the thoracic esophagus-1868 Esophagoscopy with distal light source developed around 1900

The Esophagus
E N D
Presentation Transcript
Historical Aspects • The earliest esophageal procedures were limited to the cervical region (removal of foreign bodies-1863) • Modified ureteroscope used to diagnose carcinoma of the thoracic esophagus-1868 • Esophagoscopy with distal light source developed around 1900 • Flexible fiber-optic esophagoscopy-1964
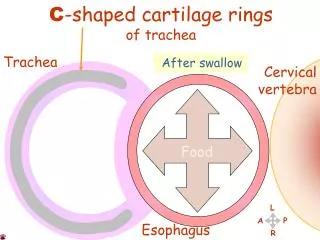
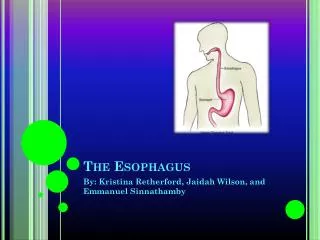
Anatomy • A hollow muscular tube approximately 25 cm in length divided into four segments • Pharyngoesophageal, Cervical, Thoracic and Abdominal • The cervical esophagus is a midline structure positioned posterior and slightly to the left of the trachea • The thoracic esophagus passes into the posterior mediastinum continuing on the left side of the mainstem bronchus and eventually enters the abdomen through the crus in the diaphragm • The abdominal esophagus attaches to the cardia (or EG junction) of the stomach (is of variable length)
Anatomy (Continued) • The esophagus has three distinct areas of naturally occurring anatomic narrowing • Cervical constriction • Bronchoaortic constriction • Diaphragmatic constriction
Anatomy (Continued) • A mucosal-lined muscular tube that lacks a serosa • It is surrounded by adventita • The adventita surrounds a coat of longitudinal muscle that overlies a inner layer of circular muscle • Between the two muscular layers is a thin intramuscular layer of fine blood vessels and ganglion cells • The upper (two-thirds) layer of muscle is striated and lower is not • The esophageal mucosa consists of squamous epithelium except for the distal 1-2 cm
Anatomy (Continued) • The esophagus has both sympathetic and parasympathetic innervation • The esophagus has an extensive lymphatic drainage that consists of two lymphatic plexuses • The esophagus has segmental blood supply and is nourished by a number of arteries
Physiology • Its basic function is to transport swallowed material from the pharynx into the stomach • Retrograde flow of gastric contents into the esophagus is prevented by the lower esophageal sphincter (LES) • Entry of air into the esophagus is prevented by the upper esophageal sphincter (UES)
Physiology (Continued) • Esophageal contractions-three types: • Primary peristalsis • Secondary peristalsis • Tertiary contractions • Esophageal peristaltic pressures range from 20-100 mm Hg with a duration of contraction between 2-4 seconds • LES-no anatomic sphincter has ever been demonstrated (resting pressures are elevated in this area)
Disorders of Esophageal Motility • Are classified as functional disorders because they interfere with a normal act of swallowing or produce dysphagia without any associated organic obstruction or extrinsic compression • Information from esophageal manometry is extremely helpful • Some conditions are indistinguishable by x-rays (barium) but have specific manometric characteristics
Disorders of Esophageal Motility • As a basic rule the tests below constitute the basic evaluation of a patient with suspected disorders of esophageal motility: • Barium swallow • Esophagoscopy • Esophageal manometry • Esophageal pH reflux testing
Disorders of Esophageal Motility • Upper esophageal sphincter dysfunction • Various (old) terms have been used: • Achalasia • Spasm • Cricopharyngeal chalasia • The terms oropharyngeal dysphagia or cricopharyngeal dysfunction better described the symptoms that occur when there’s difficulty propelling liquid or solid food from the oropharynx into the upper esophagus
Causes of Oropharyngeal Dysphagia • Neurogenic • Myogenic • Structural causes • Mechanical causes • Iatrogenic causes • Gastroesophageal reflux
Clinical Presentation • The patient complains of cervical dysphagia which is localized between the thyroid cartilage and the suprasternal notch (the classical “lump in the throat”) • Expectoration of excessive saliva is common • Intermittent hoarseness can occur • Weight loss secondary to impaired caloric intake may occur
Diagnostic Tests and Treatment • Barium swallow may be normal especially in patients with intermittent symptoms • Esophageal function studies (manometric and acid reflux testing) should be performed whenever possible • In patients with severe symptoms and no reflux, surgical intervention may be necessary • Esophagomyotomy
Motor Disorders of the Body of the Esophagus • Esophageal motor disorders range from hypomotility (achalasia) to hypermotility (diffuse spasm) • Achalasia is defined as a failure or lack of relaxation • The name focuses on the distal sphincter however the condition involves the entire esophageal body • Diffused esophageal spasm is poorly understood and poorly treated
Achalasia • The etiology is not known • The characteristic clinical, radiographic and manometric findings have occurred following a variety of situations: • Severe emotional stress • Major physical trauma • Chagas’ disease • Various animal model suggests a central or peripheral vagal nerve dysfunction resulting in the development of achalasia • The classic triad of presenting symptoms include dysphagia, regurgitation and weight loss
Achalasia (Continued) • Retrosternal pain on swallowing (odynophagia) is not characteristic • Effortless regurgitation after eating especially upon bending forward is usually not associated with a sour taste of undigested food-in contrast to acid regurgitation • Often results in recurrent respiratory symptoms due to aspiration pneumonitis • Is a premalignant esophageal lesion with carcinoma developing as a late complication in patients who have this condition an average of 15-25 years
Radiographic Appearance of Achalasia • Varies with the extent of the disease • Mild dilatation and early stages progressing to massive dilatation and tortuosity and later stages • Peristalsis is disordered in early stages and lacking in later stages • The radiographic hallmark is the distal bird beak taper of the (EG) junction
Testing • Manometric criteria of achalasia are failure of the LES to relax with swallowing and a lack of progressive peristalsis throughout the length of the esophagus • Esophagoscopy is indicated an achalasia to rule out severe retention esophagitis, carcinoma or tumor of the cardia (stomach) that mimics achalasia
Treatment • Incurable • Palliative measures • Nonsurgical • Surgical • Both are directed toward relieving the obstruction caused by the nonrelaxing LES
Nonsurgical Treatment • Early stages • Sublingual nitroglycerin • Long-acting nitrates • Calcium channel blockers • Passage of Mercury weighted bougies
Surgical Treatment • Forceful dilatation (balloon) • Esophagomyotomy
Diffuse Esophageal Spasm (DES) • Is poorly understood hypermotility disorder • Results from repetitive high amplitude esophageal contractions • The etiology is unknown • These patients typically are anxious and complain of chest pain inconsistent to eating, exertion and position • The character of pain may mimic that of angina • Symptoms are greatest during periods of emotional stress • Patients may experience slow emptying of the esophagus and obstructive symptoms are uncommon
Radiographic Findings • Frustratingly variable • Classic “corkscrew” • Beaklike taper • Increase in esophageal wall thickness
Testing • Esophagoscopy • Distal esophageal obstructing lesions may produce proximal esophageal contractions that are confused with DES • Esophageal manometry • Diagnostic when present • Classic criteria are: • Simultaneous, multiphasic, repetitive, high amplitude contractions that occur after a swallow
Treatment • Due to the lack of understanding of this condition the treatment is less than satisfactory • Antispasmodics are occasionally helpful • Response to sublingual nitroglycerin is variable
Scleroderma • Esophageal motor disturbances occur in several of the collagen vascular diseases • Dermatomyositis • Polymyositis • Lupus erythematosus • Scleroderma (extremely common) • Etiology is unknown • Characterized by induration of skin, fibrous replacement of smooth muscle of internal organs and progressive loss of visceral and cutaneous function • Disruption of esophageal peristalsis is common
Testing • Esophageal manometry and intraesophageal pH readings are the most sensitive means of detection
Treatment • Standard antireflux medicine includes H-2 blockers • Cimetidine • Ranitidine • In patients with intractable symptoms gastroesophageal reflux surgery should be considered
Esophageal Diverticula • Almost all are acquired and occur predominantly in adulthood • Are classified according to their: • Site of occurrence • Pharyngoesophageal • Parabronchial • Epiphrenic • Wall thickness • True • False • Mechanism of formation • Pulsion • Traction
Pharyngoesophageal Diverticula (Zenker) • The most common esophageal diverticulum • Occurs between the ages of 30-50 (believed to be acquired) • Arises within the inferior pharyngeal constrictor, between the oblique fibers of the thyropharyngeus muscle and the cricopharyngeus muscle • Is a pulsion diverticulum • Complaints are of cervical dysplasia, effortless regurgitation of food or pills sometimes consumed hours earlier • Sometimes a gurgling sensation in the neck after swallowing is felt
Diagnosis and Treatment • Barium swallow establishes the diagnosis • Surgery is indicated in symptomatic patients regardless of the size • It is the degree of cricopharyngeal muscle dysfunction and not the size of the diverticulum that determines the relative severity of cervical dysphagia
Midesophageal (Traction) Diverticula • Are typically associated with mediastinal granulomatous disease (TB, histoplasmosis) • They are usually small with a blunt tapered tip that points upward • These are usually an incidental finding on barium swallow • They rarely cause symptoms or require treatment • Need to be differentiated from pulsion diverticula which can also occur in this location (associated with neuromotor esophageal dysfunction)
Epiphrenic (Supradiaphragmatic) Diverticula • Generally occur within the distal 10cm of the thoracic esophagus • These are pulsion diverticula that arise due to esophageal motor dysfunction or mechanical distal obstruction • Many patients are asymptomatic when diagnosed • When symptomatic their symptoms are difficult to differentiate from: hiatal hernia, DES, achalasia, reflux esophagitis and carcinoma • Dysphagia and regurgitation are common symptoms
Diagnosis and Treatment • Diagnosis is easily made with barium swallow • Esophageal function studies should also be performed to rule out any motor disturbances • Lesions < 3 cm often require no treatment • Extreme symptomatic patients sometimes require surgical repair
Miscellaneous Condition of the Esophagus • Mallory-Weiss syndrome • During the act of forceful emesis against a closed glottis increased intra-abdominal pressure can cause a tear in the mucosa (Mallory-Weiss tear) of the esophagus at the esophagogastric junction • A transmural esophageal tear is called Boerhaave’s syndrome • A history of emesis followed by melena or hematemesis is suggestive for a Mallory-Weiss tear
Indications and Contraindications • Indications include: • Dysphagia • Reflux • Hematemesis • Atypical chest pain • Many other conditions • Contraindications: • To assess reflux symptoms that respond to medical management • A uncomplicated sliding hiatal hernia
General Considerations • The esophagoscopy should be performed after barium swallow • Bacteremia during upper GI endoscopy has been well documented therefore prophylactic antibiotic treatment should be administered • Patient should be in NPO for 6-8 hours
Complications • The minor ones: • Lacerations of the lips or tongue • Dislodgment or fracture of teeth and possible aspiration • Major complication • Esophageal perforation • Cervical esophagus (40%) • Mid esophagus (25%) • Distal esophagus (35%) • Morbidity and mortality from perforation is directly related to the time interval between the occurrence of injury, diagnosis and repair
Benign Esophageal Tumors and Cysts • Benign tumors are rare (< 1 %) • Classified in two groups • Mucosal • Extramucosal (intramural) • More useful classification: • 60% of benign neoplasms are leiomyomas • 20% are cysts • 5% are polyps • Others (< 2 percent)
Leiomyomas • Most common benign tumor of the esophagus • Intramural • Occur between 20-50 years of age with no gender preponderance • 80% occur in the middle and lower third of the esophagus, they are rare in the cervical region • Obstruction and regurgitation may occur in large lesions • Bleeding is a more common symptom of the malignant form of the tumor: leiomyosarcoma