BRAIN DAMAGE
BRAIN DAMAGE. Traumatic brain Injury (TBI) Stroke/Aneuryism Anoxia Cancer Disease Development. TBI. Common sources of Traumatic Brain Injuries. Traumatic Brain Injury (TBI) is a leading cause of death and disability among children and young adults in the United States.


BRAIN DAMAGE
E N D
Presentation Transcript
Traumatic brain Injury (TBI) • Stroke/Aneuryism • Anoxia • Cancer • Disease • Development
TBI Common sources of Traumatic Brain Injuries • Traumatic Brain Injury (TBI) is a leading cause of death and disability • among children and young adults in the United States. • Each year, an estimated 1.5 million Americans sustain a TBI. • That's 8 times the number of people diagnosed with breast cancer • and 34 times the number of new cases of HIV/AIDS each year. • As a consequence: • 50,000 people die each year. • 230,000 people are hospitalized annually and survive. • 80,000 to 90,000 people experience the onset of long-term • disability each year. • The cumulative result is that today an estimated • 5.3 million people - 2% of the U.S. population - are living with a permanent TBI-related disability. • The risk is highest among adolescents, young adults, and persons older than 75 years. The risk to males is twice the risk among females.
Typical to TBI the trauma may involve damage associated with the initial blow“Coup”
And rebound damage caused to the opposite side of the brain“contra coup”
TBI- physical effects Bruising Swelling Shearing Misalignment Anoxia necrosis
TBI is associated with contusions and hematoma That may cause brain swelling and cell death.
Unfortunately many victims of head trauma do not exhit immediate obvious symptoms -Post concussive syndromes
Case studies of PCS- Auto accident • “Melissa spent the next day spraying vomit into her bedpan and vehemently denying anything was wrong with her. She laughs and cries and rages within moments of one another and complains that she cannot see the ceiling…… • Cat scans failed to find conclusive indication of brain damage….diagnosed as PCS. • ..”..the accident shook, turned and rattled her brain, causing widespread disruptions on microscopic levels. Detailed scans a year later will reveal that Melissas brain was riddled with focal defects, pockets of arbitrarily traumatized tissue encapsulated within healthy brain. Sheering injuries in her occipital lobe disrupted key functioning in her visual cortex: diffuse axonal injuries severed untold neural connections within the right frontal lobe, compromising her self-regulation. Cellular injuries to her parietal lobe interrupted the normal processing of sensory input… • “prior to the accident , Melissa was a paragon of modern womanhood, the emodiment of every contemporary virtue. • “I was a real catch she says, gigling a little..” A master swimmer, cross-country skier, white water kayaker..had won awards in writing, public speaking. Ambition filled her veins, self-reliance and independence exuded from her smile….” • Over the course of the next days/weeks..…Melissa developed a stutter, moved about as if under sedation, had lost coordination to the point that picking up a coffee mug was a challenge, had problems of equilibrium… • ..returned to work 2 months later…fumbled with her office keys (they all looked the same to her) , could not read (understand) a memo, became lost in the hallways, forgot the names of coworkers.. • ..cried a small provocations, snapped at her assistant…
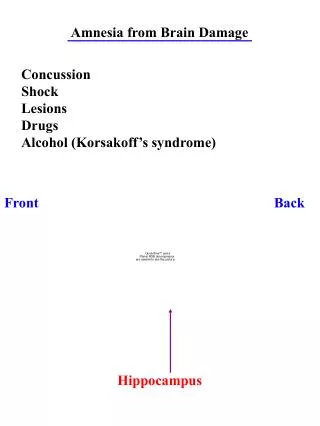
STROKE /CEREBROVASCULAR ACCIDENT Transient ischemic attack (TIA) refers to temporary brain dysfunction lasting no longer than 24 hours due to a shortage of blood and oxygen. It sometimes is referred to as a "mini-stroke." TIA is a serious condition that serves as a warning for a stroke. About 30% of stroke patients have had a TIA at some point in the past. Stroke/cerebrovascular accident (CVA) is a brain injury that occurs when the brain's blood supply is interrupted. Without oxygen and nutrients from blood, brain tissue starts to die rapidly (usually in less than 10 minutes), resulting in a sudden loss of function.
Risk Factorsfor Stroke • High blood pressure (the number one risk factor for ischemic stroke) • Drug abuse (heroin, cocaine , amphetamines) • Narrowing of arteries supplying the brain due to atherosclerosis • High cholesterol levels , particularly low-density lipoprotein (LDL) cholesterol • Smoking • Diabetes mellitus • Atrial fibrillation (abnormality of heart rhythm) • Use of birth control pills if you are over 35 years old and smoke • Long-term use of hormone replacement therapy*²
Symptomsof Stroke- • Visual disturbances like blindness in one eye, and/or blurry, dimming or double vision. • Weakness, numbness, or tingling of the face, arm, leg, or one side of the body (usually affects one side of the body, but there are exceptions). • Difficulty speaking or understanding words • Difficulty swallowing • Dizziness, unsteadiness of gait, loss of balance or falling • Trouble with balance or coordination • Loss of consciousness • Nausea and/or vomiting • Sudden confusion or loss of memory • Seizures • Severe or unusual headache
Brain stem stroke damage resulting from partial occlusion of the pontine arteries and basilar artery and complete occlusion of one pontine artery. Tissue damage due to lack of blood supply of the pontine area of the brain stem is a cause of locked-in syndrome (basilar artery syndrome).
Persistent vegetative State (PVS) syndromes vs. “Locked in Syndrome” Locked-in syndrome: (Severe brainstem injuries) individual is alert but can not control movement or function…except sometimes eyeblinks (the waking nightmare). PVS: severe cortical damage leaves patient without consciousness, but subcortical processess are intact so that eating, drinking, even laughing/crying may occur as reflexive/automatic behaviors (waking death).
RX for Stroke? • MedicationsClot-dissolving drugs—given within three hours of the onset of symptoms. (Note: Only in carefully selected patients.) Tissue plasminogen activator (tPA) is given through a vein after the doctor has confirmed the stroke's cause and there is no evidence of bleeding. • Blood-thinning drugs (Anticoagulants)—Clexane is given by subcutaneously (along with tPA, if indicated) and an oral medication (warfarin) is sometimes started if long-term treatment with a blood-thinner is anticipated. • Antiplatelet drug— aspirin is the most common, but clopidogrel (Plavix), dipyridamole (Persantine) are also sometimes used. • Blood pressure medication(usually use Labetalol, the first-line drug, or sodium nitroprusside) • Diabetes mellitus medication • Drugs that reduce brain swelling • Medication to control or correct irregular heart rhythm (such as atrial fibrillation) • Cholesterol-lowering medications • Other interventions during an acute stroke include: Providing adequate oxygenTaking precautions to prevent chokingFrequent neurological examinations
Deep brain stimulation for comatose victims of brain damage?
Brain Neoplasms • Types of Primary Brain Tumors • Primary brain tumors arise from the tissues of the CNS - rather than originating from cancerous cells that travel from elsewhere in the body. • Primary brain tumors are categorized as either benign (noncancerous) or malignant (cancerous). • noncancerous primary brain tumors still can have devastating physical and emotional effects. • For most patients, there generally is no obvious exposure or risk factor that can be linked to these tumors.
Until recently, many brain tumors were considered inoperable. The tumors were either so deep that conventional surgery to completely remove them would damage critical parts of the brain, or the tumors were so densely entangled with blood vessels that surgery would likely cause a fatal brain hemorrhage. Fortunately, scientists have discovered a high-tech, non-invasive tool that makes such risky surgeries far less dangerous. Photon surgery is a form of stereotactic radiosurgery -- that is, a non-invasive treatment of precisely focused X-rays used to treat brain tumors.
Bacterial and Viral Infections of the Brain • Following are descriptions of some bacterial and viral infections. • I do not require that you memorize specific bacterial or viral infections. You should recognize that this is a meaningful source of damage to the CNS.
Bacterial Meningitis • Certain bacteria can cause an infection in the meninges. a serious infection that can cause death within hours. • Causes • The bacteria first cause an upper respiratory tract infection . Then it travels through the blood stream to the brain. • You do not need to memorize these, but you may be interested: Streptococcus pneumoniae (the bacteria that causes pneumonia ) • Neisseriameningitidis • Haemophilusinfluenzae b (Hib) • In the US, widespread immunization has almost eliminated meningitis due to Hib Listeriamonocytogenes meningitis • Escherichia coli meningitis , • Mycobacterium tuberculosis meningitis • In general, meningitis is not spread by casual contact.
Symptomscan develop over several hours, or 1 to 2 days: High fever Headache Very stiff, sore neckOther symptoms may include: Red or purple skin rash Cyanosis (bluish skin color) Nausea Vomiting Photophobia (sensitivity to bright lights) Sleepiness Mental confusion
Rabies virus • Rabies is an infectious disease of animals. Man is occasionally infected, and once infection is established in the CNS, the outcome is almost invariably fatal. • HUMAN RABIESIs acquired from virus in saliva entering a bite wound caused by an infected animal, usually a rabid dog. The severity of the bite determines the risk of infection. The disease does not usually spread from man to man. • IncubationAfter inoculation, the virus enters small nerve endings at the site of the bite. The virus slowly travels up the nerve to reach the CNS where it replicates and then travels down nerves to the salivary glands where there is further replication. The incubation period may last from two weeks to six months. Very often the primary wound is healed and forgotten by the time of clinical presentation. • Clinical PresentationA) Furious Rabiesheadache, fever, irritability, restlessness and anxiety. This may progress to muscle pains, salivation and vomiting. After a few days to a week the patient may experience a stage of excitement and be wracked with painful muscle spasms, triggered sometimes by swallowing of saliva or water. The stage of excitement lasts only a few days before the patient lapses into coma and death. Once clinical disease manifests, there is a rapid, relentless progression to invariable death, despite all treatment. • B) Dumb RabiesStarts in the same way, but instead of progressing into excitement, the subject retreats steadily and quietly downhill, with some paralysis, to death. Rabies diagnosis may easily be missed.
Viral meningitis A relatively mild disease with a good prognosis. Patients present with fever, headache, neck stiffness and photophobia. Common viral agents include: enteroviruses, mumps virus and lymphocytic choriomeningitis virus. Acute necrotizing encephalitis Infection of the brain by HSV. Neurons of the temporal lobe are most commonly involved. Infection is severe and necrotising. Clinical features include: sudden onset of fever, headache, confusion and alteration in personality. Mortality is high and neurological impairment in the survivors is invariable. Encephalitis may be due to primary infection or reactivation.
Progressive multifocal leuco-encephalopathy The Papovavirus family contains two main groups:-Papilloma viruses (which cause warts)Polyoma viruses, these are slightly smaller than papilloma viruses, and in animals are sometimes associated with tumours. The two known human polyoma viruses are: JC - Progressive multifocal leuco-encephalopathy BK - isolated from urine of immunosuppressed patients dsDNA genome small icosahedral particles, 42-45 nm grows in human foetal glial cell cultures (JC) Progressive multifocal leuco-encephalopathy is a progressive neurological disorder caused by reactivation of JC virus in the brain. Infection is common, but neurological disease is rare; it only occurs in immunosuppressed patients. Clinical FeaturesPatients may present with a variety of neurological signs, including: hemiparesis, dementia, dysphagia, muscular inco-ordination or impaired vision. The condition is progressive and invariably fatal. PathologyMultiple foci of demyelination are found throughout the cerebral hemispheres and cerebellum. The virus infects oligodendrocytes, which have a bizzare histological appearance. EpidemiologyInfection with JC virus is common, but invariably asymptomatic: Seroprevalence surveys have shown that about 50-60% of adults have antibodies.
Retrovirus DiseaseLentivirinae: Lentivirusescharacteristically establish a persistent infection in the host and cause chronic wasting disorders which are uniformly fatal. PathologyInflammatory cell infiltration, perivascular cuffing of blood vessels, demyelination, necrosis and reactive gliosis.
Kuru This is a transmissable prion disease found only in the Fore people of New Guinea. It first appeared about 60 years ago and the incidence increased until the late 1950's. The disease is now known to have been transmitted through ritual cannibalism: until the late 1950's it was the practice of women and children to eat the brains and viscera of dead relatives, including those who had themselves died of Kuru. Cannibalism stopped in 1957 and the incidence of Kuru has declined sharply since then. Clinical features:The incubation period varied from 4-20 years. Patients presented with progressive cerebellar dysfunction. Death usually occurred within a year of initial presentation. Transmission studies:Intra-cerebral inoculation of brain tissue from Kuru victims into non human primates leads to the development of symptoms within two years.
Creutzfeldt-Jakob disease (CJD)In 1920, Creutzfeldt described a progressive dementing illness in a 22 year old woman. The following year, Jakob described four older patients with a clinically similar presentation and course. Since then, numerous cases of CJD have been described. CJD occurs world wide. It is very rare, with an incidence of about 1 case per million population. While most cases are sporadic, 5-10% are familial. In the familial form, CJD is inherited as an autosomal dominant condition. Clinical featuresThe onset of the disease typically occurs between the ages of 50 and 65 years. There are two main modes of presentation: 1. Chronic dementing illness 2. Progressive cerebellar dysfunction The condition is relentlessly progressive and patients usually die within a year of presentation. Transmission:The natural route of infection is not known, but CJD has been accidently transmitted by:1. Corneal grafts - where the corneas were harvested from cadavers that died of CJD.2. Growth hormone preparations, derived from human pituitary glands.3. In two patients who received grafts of dura mater, prepared from cadavers, and4. through electrodes used for electro-encephalography which had previously been used in a patient with CJD. The prion detected in the brains of patients with CJD is termed PrPCJD. The disease has also been experimentally transmitted to chimpanzees and other primates. Following intracerebral inoculation, the incubation period is 11-14 months. The disease can also be transmitted peripherally (IV, intra peritoneal or intramuscular routes). But transmission is much less efficient and the incubation period is much longer (many years).
General Functional Effects of Brain damage-largely depend on what brain region is involved-You should be able to characterize the following deficits: • Anomias • Functional deafness • Aprosodias • Asomatognosia • Unilateral neglect • VIsual hemi-neglect • Apraxias • hemiplegia • Amnesias • Changes in Affect • Loss of Judgement • Impulsivity • Bizarre behaviors • Aphasias • Anosagnosias • Etc...
Brainstem syndromes • Wallenbergs (lateral medullary): CN5 (ipsilateral facial analgesia), 8 (vertigo), 9, 10 (hoarse,etc), sympathetics (ipsilateral Horner’s), solitary nuc. (taste), cuneate/gracile nuc. (ipsilateral numbness), spinothalamic tract (contralateral pain/ temp loss – only 1 contralateral); no weakness • Webers: ventral midbrain; CN3 w/crossed hemiplegia • Claude: dorsal midbrain; CN3 w/ataxia • Benedikts: CN3 w/ ataxia and hemiplegia • Parinauds: upgaze palsy, loss of accomodation (fixed pupils) – only 1, large pupils w/ light/ near dissociation, convergence nystagmus, nystagmus retractorius, lid retraction • Millard-Gubler: base of pons, CN6 & 7 and contralateral hemiplegia • Medial medullary: contralat hemiparesis (not face), contralat numbness, ipsi CN12 • Lateral pontine (SCA): ipsi ataxia, contralat pain/temp, deafness, N/V • Locked-in: Bilateral basilar pons • Pseudobulbar palsy: lesion of bilateral UMN corticobulbar tracts above brainstem (eg IC); unable to move eyes, mouth but can yawn & cry (reflexive). Brisk jaw-jerk/reflexes. Also frontal signs, emotional lability may occur due to adjacent frontal fiber damage. • Bulbar palsy: LMN CN palsy (usu IX-XII) • Top-of-the-Basilar: sudden onset AMS, EOM/ pupil/ visual (homonymous hemianopsia) abnormalities, usu. Embolic. • Brainstem Reflexes: • Pupil = 2 & 3. • Dolls = 3 & 8 (VestNuc > PPRF > CN3/6). • Jaw-jerk = 5 only. • Corneal = 5 & 7. • Pupillary = 2 & 3. • Gag = 9 & 10. • Cough = 10 only. • Oculocardiac: V1 to X.