Sympathetic Pain
590 likes | 807 Vues
Sympathetic Pain. By Dr, Salah Ibrahim 2012. Sympathetic system arises from the spinal cord between 1 st thoracic and 2 nd lumbar segments The cells of the preganglionic fibers lie in the intermediolateral column of the spinal cord.

Sympathetic Pain
E N D
Presentation Transcript
Sympathetic Pain By Dr, Salah Ibrahim 2012
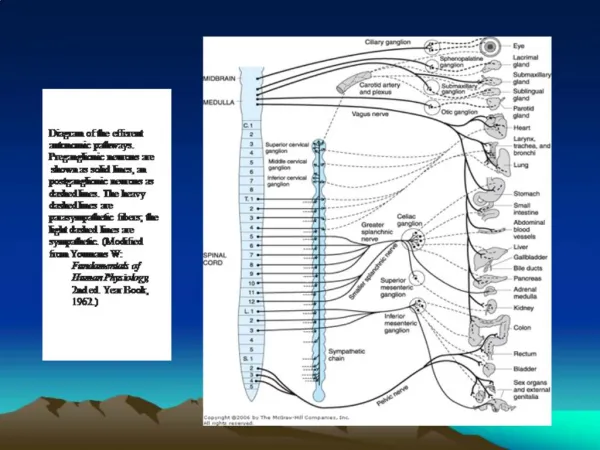
Sympathetic system arises from the spinal cord between 1st thoracic and 2nd lumbar segments The cells of the preganglionic fibers lie in the intermediolateral column of the spinal cord
The preganglionic fibers leave the spinal cord via ventral roots then leave the spinal nerve as a white ramus to join sympathetic ganglia Each ganglia in the sympathetic chain is connected to one spinal nerve by grey ramus There are 14 white rami (12 thoracic and 2 lumbar) and 31 grey rami (31 spinal nerves)
The preganglionic fibers in the white ramus may synapse with cells in the ganglion, may pass upwards or downwards or may not synapse at all and continue as preganglionic fiber called splanchnic nerves. The splanchnic nerves leave the chain and pierce the diaphragm to synapse with coeliac, superior and inferior hypogastric ganglia The post ganglionic fibers from these ganglia form extensive plexus around the big vessels
There are two sympathetic chains. Each chain extends from the level of the 1st cervical vertebrae to the front of the coccyx where both unite to form ganglion impar • The preganglionic fibers from the upper thoracic segments run upward to synapse with three cervical ganglia. The postganglionic fibers leave these ganglia as grey ramus to the cervical nerves • The same occurs for thoracic, lumbar and sacral nerves.
The sympathetic system shows a widespread distribution of postganglionic fibers from a single white ramus, therefore stimulation of a single white ramus will have a widespread effect (mass effect or fight and flight response) On the other hand the postganglionic parasympathetic fibers have only a short and direct course to the effector cell and thus have a local and discrete response.
What are the nerves which leave the chain? • Gray ramus, which leave the lateral side of the chain. The postganglionic fibers of each grey ramus are distributed via the spinal nerve to sweat glands, hairs and blood vessels of the corresponding segments • Sympathetic visceral nerves, which leave the medial side of the chain e.g. internal and external carotid nerves, cardiac nerves, greater and lesser splanchnic nerves and lumbar splanchnic nerve
Remember that • The three cervical ganglia as well as the 2nd, 3rd and 4th thoracic ganglia supply postganglionic fibers to visceral structures in the head and thorax • The coeliac, superior and inferior hypogastric ganglia supply postganglionic fibers to visceral organs in the abdomen and pelvis.
Interruption of sympathetic nerve fibers could be achieved by :- • Intradurally or extradurally by blocking the preganglionic fibers by intra or extradural blockade • At the sympathetic chain by sympathetic paravertebral blockade
There are 3 general ways to block sympathetic nerves clinically while preserving the somatic function • To block sympathetic nerves with the same LA agents (in similar conc) used for somatic block in areas where the sympathetic fibers are separated from the somatic nerve fibers (e.g Stellate, Coeliac etc..) • To block sympathetic nerve at locations that combine somatic and sympathetic fibers but at a low conc of LA (e.g epidural especially if we can insert a catheter) • To use sympathetic antagonist (e.g use of guanethidine, ismelin in vasculature of a limb (e.g Bier technique)
Diagnostic block: is done to differintiate between visceral block and somatic block to establish the correct route of pain transmission Therapeutic block: Is obtained by either serial injection of local anaesthetic or by injection of a neurolytic agent, the goal of sympathetic blockade is to preserve motor function and touch while selectively blocking the sympathetic fibers
Indications of sympathetic blockade: • Visceral pain • Complex regional pain syndromes • Phantom limb • Post herpetic neuralgia Other indications include ischemic syndromes of the limbs, myofacial pain and neuropathies
(1) Visceral pain Viscerla pain is transmitted through afferent fibers that run in sympathetic nerves. There are small, unmylinated fibers and can transmit burning or colicky sensations. Their bodies are situated in DRG they are conveyed together with somatic noxious stimuli via the spinothalamic and spinoreticular tract to the brain
The afferent fibers may synapse with interneurone in the intermediolateral part of the spinal cord to pass through the efferent preganglionic sympathetic fibers to reach the viscera. There is also a synaptic connection with efferent to the skeletal muscle Thus producing a positive feedback loop giving self sustained pain. This loop effect will increase the sympathetic tone that may lead to serious effects especially in cardiac patients
About 15-20% of the afferent visceral unmylinated fibers do not go through the dorsal root but turn back from the dorsal root to enter via the ventral root. Dorsal rhizotomy does not always relief chronic visceral and pelvis pain successfully
Visceral afferent running in sympathetic nerves inflow to the throacolumbar spinal cord (T1-L2) constitute only less than 10% of the total inflow to this part of the spinal cord. The remaining 90% is coming from the somatic parts (areas of the back and abdomen). So GIT has a low sensory innervation and this explains why large areas of the gut appear insensitive to pain
Visceral pain is almost always referred The somatic and visceral afferents converge to the same spinothalamic neurone. Since somatic pain is much more represented than visceral pain. Therefore, any visceral pain will be projected to the same somatic area and will be felt in a particular peripheral structure
Types of nociceptive convergence (1) Viscerosomatic convergence: Visceral sensations are mediated only through convergence with the somatosensory pathway (2) Viscero-visceral convergence: In which the 2nd order neurone receive input from two or more viscera. There is augmentation of pain symptoms between the two viscera that share the afferent supply (e.g patients with coronary heart disease and gall bladder sharing the afferent pathway of T5)
Role of sympathetic efferent fibers Their role in the production of visceral pain cannot be excluded in the mechanism of visceral pain The use of the different α– adrenergic blocking drugs may produce visceral pain relief of moderate quality
Although opioids given in appropriate doses can give some relief of pain, yet sympathetic blockade will give good relief because of blockade of the afferent sympathetic pathway from visceral structures. Moreover the interruption of the afferent and efferent limbs of the viscero-somatic and viscero-visceral reflexes will prevent the feedback loop which is responsible for sustained pain and increase of sympathetic tone
Sympathetic blocks for visceral pain • Pain in visceral structure in head, neck and upper thorax Stellate block • Pain from thoracic structures Epidural block • Pain from upper GIT coeliac plexus block • Pain from lower abdomen Lumbar plexus block • Pain from abdomen and pelvis Superior hypogastric block • Perianal pain Ganglion impar block (Walther)
Factors capable of inducing visceral pain • Abdominal distention • Contraction of hollow viscus • Rapid stretching of capsule of solid organ • Ischemia of viscera • Accumulation of inflammatory mediators • Traction of mesentery • No cutting – No crushing – No cauterization
Visceral pain is felt along the central throacolumbar axis of the body (low sternal and upper epigastrium) , is vague, dull, has oppressive quality and of high intensity accompanied with pallor, sweating, nausea or vomiting. After a period of few minutes or few hours, the pain stops and becomes referred to a parietal structure where it becomes sharp in quality and is clearly localized in the referred area
(2) Complex Regional Pain Syndrome SMP, sympathetic mediated pain is that aspect of pain that is maintained by efferent sympathetic activity or circulating catecholamines and that respond to sympathetic blockade SMP, may be a component of many different painful conditions but is not essential requirement for any painful condition
Patient A: whose pain is only 20% sympathetically maintained and 80% sympathetically independent (SIP) Patient B: whose pain is 80% sympathetically maintained and exhibit SMP B SMP A SIP
CRPS It’s a syndrome of pain with regional distribution and having complex nature
Criteria of diagnosis of CRPS There is PAIN plus • Sensory changes (allodynia and hyperalgesia) • Vasomotor changes (Temp, color changes) • Sudomotor changes (Sweating of affected limb) • Oedema (of affected limb) • Motor and trophic changes (Weakness, hair loss, nail changes)
The ability to differentiate CRPS from other neuropathic pain syndrome by the presence of oedema, vasomotor and sudomotor changes
The fact that the somatosensory symptoms of type II extend beyond the course of the affected nerve distinguish this syndrome from isolated peripheral mononeuropathy
Confirmatory tests to detect abnormalities in sympathetic activity • Thermography (difference of 1°C is considered significant) • X-ray reflect ground glass appearance of the bone of affected limb (osteopenia) • Abnormal uptake of 99mTc in the bone of the painful extremity • When sympathetic blockade produces pain relief • IV phentolamine infusion test (1mg/kg) over 10 minutes produces pain relief (clue of diagnosis of SMP)
Mechanism of SMP • The sympathetic – sensory coupling (s-s coupling) According to the coupling mechanism, the sympathetic efferent and the sensory afferent are no longer separated. Therefore, activity in the sympathetic neurons may lead to continuous activity of α1 adrenergic receptors of afferent sensory fibers generating continuous pain (notice importance the use of α1 adrenergic blockers)
Cont. of S-S coupling Notice: activations of α2 adrenergic receptors located in sympathetic terminals block the release of NE and so it relieves sympathetic pain (clonidine) The continuous spontaneous pain may cause sensitization of the dorsal horn neurons resulting in the various forms of abnormal sensation and the wide radiation of the clinical features of CRPS after the inciting cause has healed or removed
(2) Another theory proposed that it was found in rats that following peripheral nerve injury, sprouting occurs in the postganglionic sympathetic fibers around the sensory neurons in the DRG and represent another potential site of direct coupling between sensory and sympathetic efferent fibers Remember: This S-S coupling can explain the mechanism of CRPS type II and CRPS type I with nerve lesion
(3) The occurrence of pain in CRPS type I without nerve lesion could be explained by the occurrence of cutaneous inflammation, the inflammatory process being augmented by α1 receptor function The released NE might lead to cutaneous vasoconstriction and the release of PGE2 secondary to release of NE. This theory is supported by that fact that this pain is significantly reduced after the injection of indomethacin
3- Phantom limb pain Phantom limb is an intermittent pain with variable duration from minutes to few hours, the pain is felt in the distal part of the missing limb The pain might be :- • Shooting, electric like (neuroma formation) • Throbbing, burning (sympathetic activation) - Squeezing or cramping (increased muscle tension)
Proof that sympathetic activation may help in development of phantom pain: • Is that exacerbation of phantom pain by stress and emotional states that resulted from increased catecholamines release from the sympathetic efferent terminals which are in close proximity to sprouts and afferent fibers • Also phantom pain is evoked after injection of NE in the stump end
However in cases where there is throbbing and burning pain with lower temperature of the residual limb compared with the sound limb, you can perform sympathetic block to increase blood flow to the residual limb with significant pain relief