Sympathetic Drugs
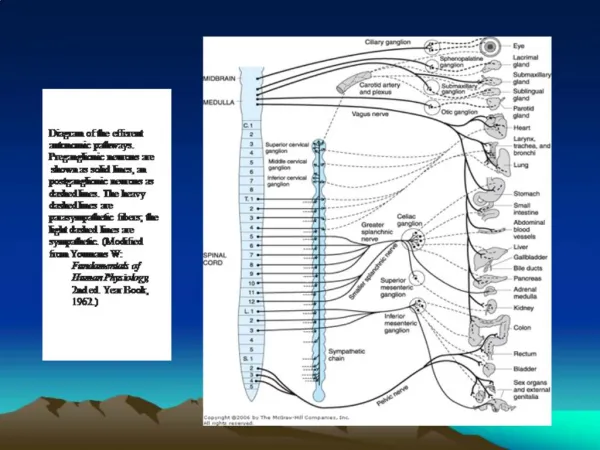
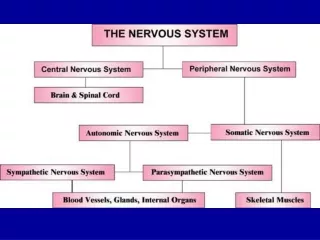
Sympathetic Drugs. Stress and The Adrenal Glands. Adrenal Medulla: A Modified Sympathetic Ganglion. Mechanism: Norepinephrine Release and Recycling. Review of Efferent Pathways: Motor and Autonomic. Catechalomines: Activity. Stimulates the “fight or fight” reaction

Sympathetic Drugs
E N D
Presentation Transcript
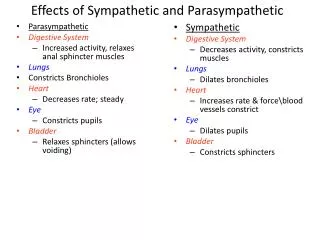
Catechalomines: Activity • Stimulates the “fight or fight” reaction • Increased plasma glucose levels • Increased cardiovascular function • Increased metabolic function • Decreased gastrointestinal and genitourinary function
Sympathomimetics • Drugs that partially or completely mimic the actions or norepinephrine (NE) and epinephrine (Epi). • Act either - directly on α- and/or β- adrenoceptors or indirectly on presynaptic terminals, usually by causing the release of NE. • See Below
β2-Adrenoceptor Agonists – cause bronchial dilation - used for the treating asthma, prevent pre-term labor (relaxing uterine muscle). • β1-Adrenoceptor Agonists – (e.g., dobutamine) sometimes used to increase the force of heart contraction in severe low-output heart failure. • α1-Agonists – (e.g., phenylephrine) – used as mydriatics, decongestants. • α2-Agonists – (e.g., clonidine, methyldopa) – centrally acting hypotensive drugs.
Sympathomimetics act mainly by causing release of NE (e.g., amphetamine) have the α1/α2 selectivity of NE. • β-Adrenoceptor antagonists (β-blockers) – used to treat hypertension, angina, cardiac arrhythmias, CHF, and glaucoma. • α-Adrenoceptor antagonists (α-blockers) – limited clinical application – prazosin (selective α1-antagonist – used to treat hypertension. • Adrenergic neuron blocking drugs – either deplete the nerve terminals of NE or prevent its release – used as hypotensive agents.
Metabolism of Norepinephrine
Reuptake • Monoamine Oxidase • Catechol-O-methytransferase (COMT) • α1-Adrenoceptors – in several tissues (e.g., smooth muscle, salivary glands) incr IP3 and [Ca2+]in vasoconstriction or glandular secretion • α2-Adrenoceptors – on noradrenergic nerve terminals. Activation by NE inhibit AC, decrcAMP, Ca2+ channels close decr further nt release. • β-Adrenoceptor – stim AC incr [cAMP] 2nd messenger intracellular signaling physiol response.
Indirectly-Acting Sympathomimetics • Transported into nerve terminals where they displace vesicular NE into the cytoplasm. Some is metabolized by MAO, but the remainder is released by carrier-mediated transport to activate adrenoceptors. • Amphetamines – resistant to MAO. - Peripheral actions - tachycardia, hypertension - mainly caused by catecholamine release. - Dexamfetamine and methylphenidate used for hyperactive children. • Cocaine – NE reuptake inhibitor (also dopamine) – Intense central stimulant popular drug of abuse.
Acute and chronic effects of Indirectly acting sympathomimetics G = Guanethidine
Mechanism of action of cocaine and reserpine
Directly-Acting Sympathomimetics • Effects in humans depends on their receptor specificity (αand/or β) and on the compensatory reflexes they evoke. • Epiincrbp by stim the rate and force of the heart beat (β1 effects). • Stimulation of vascular α-receptors causes vasoconstriction (viscera, skin), whereas…, • Stimulation of vascular β2-receptors vasodilation (skeletal muscle) … • And the total peripheral resistance may actually decrease. • NE has little-to-no effect on the vascular β2-receptors; thus, the α-mediated vasoconstriction is unopposed. • The resulting rise in bp reflexively slows the heart, usually overcoming the direct β1-stimulant action on the heart rate.
β-Receptor-Selective Drugs • Isoprenaline – stimulates all β-receptors incr rate and force of heart beat and vasodilation full diastole and MAP, with little change in systolic pressure. • β2-Adrenoceptor Agonists – relatively selective class of drugs that produce bronchodilation – used for asthma (resistant to MAO, not uptaken into neurons).
Adrenoceptor Antagonistsα-Blockers • Decrartiolar and venous tone decr peripheral resistance hypotension. • Reverse the pressor effects of Epi, because its β2-mediated vasodilator effects are unopposed by α-mediated vasoconstriction peripheral resistance falls (Epi reversal). • Cause reflex tachycardia – this is greater with non-selective drugs that also block α2-presynaptic receptors on the heart, because the augmented release of NE further stimulates the cardiac β-receptors (e.g., prazosin).
Adrenoceptor Antagonistsβ-Blockers • Vary in lipid solubility and cardioselectivity • All block β1-receptors and decrbp and prevent angina. • Higher Kow-drugs more rapid absorption from GIT, 1st-pass hepatic elimination more rapidly eliminated. • Also more likely to enter CNS and cause central effects (e.g., nightmares). • Cardioselectivity diminishes with higher doses.
Adrenoceptor Antagonistsβ-Blockers (Cont’d) • Nevertheless, selective β1-blockade less peripheral vasoconstriction (cold hands and feet) and does not reduce the response to exercise-induced hypoglycemia (stim of gluconeogenesis in liver is mediated by β2-receptors). • Cardioselective drugs may have sufficient β2-activity to ppt severe bronchospasms in patients with asthma – these patients should avoid β-blockers . • Some possess intrinsic sympathomimetic activity (partial agonists), but this is debatable.
Catecholamine synthesis, storage, release, and reuptake pathways