CABG VS Multi Vessel PCI
CABG VS Multi Vessel PCI. Hasanat Sharif MD FRCS Chief of Cardiorthoracic Surgery Aga Khan University Hospital. Multivessel. Definition Cardiologist Cardiac Surgeon. Treatment of Coronary Artery Disease. Medical Percutaneous Intervention Surgical Revascularization.

CABG VS Multi Vessel PCI
E N D
Presentation Transcript
CABG VSMulti Vessel PCI Hasanat Sharif MD FRCS Chief of Cardiorthoracic Surgery Aga Khan University Hospital
Multivessel • Definition • Cardiologist • Cardiac Surgeon
Treatment of Coronary Artery Disease • Medical • Percutaneous Intervention • Surgical Revascularization
Treatment of Coronary Artery Disease • Medical • Advances in medical treatment • Anti platelet agents • ACEI/ARB • Statins • Aggressive risk factor modification
Treatment of Coronary Artery Disease • Primary percutaneous intervention • Role in evolving acute myocardial infarction • Culprit vessel addressed
Intervention • Interventionalist’s procedural bias • Perception • Clinician • Referring doctors and • Patient
Two-year outcomes for SYNTAX Kappetein AP. European Society of Cardiology 2009 Congress; September 2, 2009: Barcelona, Spain.
Approriateness criteria for coronary revascularization • Refined and extended guidance beyond that provided by evidence based guidelines • Expert panel of 17 members • Year long effort to evaluate available evidence and existing guidelines
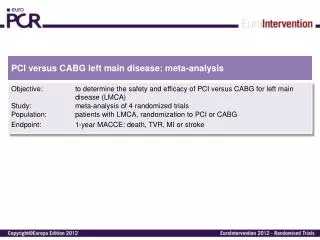
Appropriateness Criteria • Inappropriate 1-3 • Uncertain 4-6 • Appropriate 7-9 • PCI inappropriate for LM CAD • PCI uncertain for 3 VCAD • PCI appropriate for acute myocardial injury • CABG appropriate for 3VCAD and LM CAD
What happens in actual practice? • Catheterization laboratory cardiologists in hospitals with PCI capability were more likely to recommend patients for PCI than • Hospitals in which only catheterization was performed
Indicated CABG 13% PCI 59% Both 17% Recommended 53% (34% PCI) 94% 93% PCI 5% CABG Adherence to ACC/AHA guidelines
Trials • Justification • ? Economically/industry driven • ? Extending the boundaries of care • Randomization • Multi centered • Adequate numbers • Long term follow up • End point - survival
Trials • Ethics • Informed patient consent • Critical to provide complete disclosure of risks/benefits • Survival • Stent thrombosis/graft closure • Risk of re intervention/complications
Trials • Enrolled only 5-10% of the eligible population • ? Generalizability of results • Real life situations
Trials • Propensity analysis is not perfect • Euroscore over predicts procedural risk • Cost analysis and impact on healthcare budget
Observational data • Consistently show a survival advantage for CABG over PCI • STS database • Northern New England database • Duke • New York
AKU Data Fifty month data Jan 2006-March 2010 • Total CABG n=2041 • Left main n= 406 (19.9%) • 1 VCAD n= 69 (3.4%) • 2 VCAD n= 257 (12.6%) • 3 VCAD n= 1715 (84%)
AKU Data • Mean age 58 years (+/-11) • Males 82% • LVEF 48% (+/-14) • IMA usage 90% • CVA n = 8 (0.4%) • Mortality n = 32 (1.6%)
Cost Considerations • CABG package 225K • One bare metal stent 285K • Additional stent 32K • One DES 395K • Additional stent 139K
Triple vessel and left main coronary stenosis • CABG first choice for majority of patients • Consider PCI for patients with co morbidities that preclude CABG • Advances • PCI technology and • Surgical techniques/ peri operative care • Extending the boundaries of cardiovascular care
Treatment of coronary artery disease • Multidisciplinary team approach • Cardiologist • Interventionalist • Cardiac Surgeon • Separate diagnosis from treatment! • Treatment option given on cath table • Scare tactics