DENGUE FEVER
440 likes | 889 Vues
DENGUE FEVER. Prof. Dr. Muhammad Ali Khan MBBS, DCH, MRCP (UK) Secretary DEAG Punjab Ex Head Department of Pediatrics SIMS/Services Hospital Lahore. Dengue Virus. Family : Flaviviridae Genus : Flavivirus Serotypes : DV1, DV2, DV3, DV4 Enveloped virus 3 major proteins

DENGUE FEVER
E N D
Presentation Transcript
DENGUE FEVER Prof. Dr. Muhammad Ali Khan MBBS, DCH, MRCP (UK) Secretary DEAG Punjab Ex Head Department of Pediatrics SIMS/Services Hospital Lahore
Dengue Virus Family : Flaviviridae Genus : Flavivirus Serotypes : DV1, DV2, DV3, DV4 Enveloped virus 3 major proteins SS positive sense RNA Dr. S Guanasena
Viral Serotypes DV1 DV2 DV3 DV4 Subgroups and clades One or more virus types in circulation during an epidemic
Dengue Infection Clinically significant Dengue infection may be 1. Simple dengue fever (DF) 2. Dengue hemorrhagic fever (DHF) (plasma leak <5%) 3. Dengue Shock Syndrome (DSS) (plasma leak >5%)
Clinical Features – DF • Fever > 2 and < 10 days (essential criterion) • Headache • Retro orbital pain • Myalgia • Arthralgia/ severe backache/ bone pains • Rash • Bleeding manifestations (epistaxis, hematemesis, bloody stools, menorrhagia, hemoptysis) • Abdominal pain • Decreased urinary output despite adequate fluid intake • Irritability in infants
DHF or DLF
SHOCK A complex clinical syndrome of decreased blood flow to body tissues resulting in cellular dysfunction and eventual organ failure
Plasma leaks - Pathophysiology • Host response • Subsequent infection • Previous IgG • Neutralizing (protective) • non neutralizing (replication enhancing) • Increased viremia increased TNF, interferon, interleukin-2 and hypocomplementemia endothelial injury and increased leakage • Viral response
Pathophysiology of DHF • Increased capillary permeability • Protein rich fluid exudes into the interstitial space - Pleural effusion , Ascites etc. • Circulatory volume collapses – SHOCK • Sympathetic over activity • Vasoconstriction, tachycardia • Loss of volume • Reduces pulse pressure • Blood becomes thick due to loss of fluid • Rising hematocrit and delayed capillary filling • Compromised renal and hepatic perfusion – • Reduced urine output and tender hepatomegaly
Patho-physiology of DHF Management of DHF during the critical stage is that of Shock But there is one important consideration: Fluid is not being lost out but it is going to 3rd space and will be resorbed back so Over-enthusiastic fluid replacement during the critical phase – when the fluid is oozing out - would result in fluid over load during the recovery phase
Patho-physiology of DHF • Peopledo not die of hemorrhage in DHF • They die • Either due toshock and 20 organ failure • Or due to Pulmonary edema & fluid over loadduring the recovery phase
End organ failure in DHF Approximate outcomes Single organ failure - mortality = 40% Two organ Failure - mortality = 80% Three organ failure - mortality = >99%
Case review ( of 9 deaths at Services Hospital ) 8 died of profound shockand associated end organ failure Only one had suspected CVA as a cause of death
Clinical course of DHF Course of simple Dengue fever is generally uneventful and non-fatal Whereas DHF can be life-threatening Differentiating DF from DHF is critical
Clinical course of DHF • Both the DF and DHFcan have bleeding tendencies therefore: Bleeding is not the differentiating point between the two
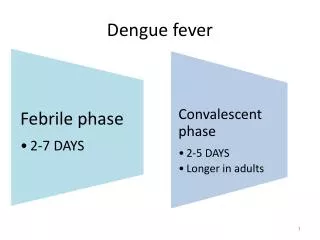
Clinical course of DHF Clinical course can be divided into three stages Febrile Phase Critical Phase Recovery Phase
Clinical course of DHF Febrile Phase High fever Some petechial hemorrhages With generalized aches & pains and headache; this usually lasts two to seven days People generally don’t die during this stage
Clinical course of DHF Critical Phase Starts with the resolution of fever Occurs in a few people Lasts for just 24-48 hours or so Is associated with plasma leak – volume depletion & shock This is the phase where management is critical
Clinical course of DHF DHF is classically associated with Plasma leakinto the 3rd compartment And circulatory compromise
Signs of plasma leak in DHF Patient is not feeling well with resolution of fever Warning signs Low pulse pressure <20 mm Low urine output Delayed capillary filling Tender hepatomegaly
Signs of impending DHF Warning signs (lab reports) Increasing hematocrit Edema of the gall bladder, ascites or pleural effusion Low albumin Low cholesterol Acute fall in platelet count
Clinical course of DHF Recovery Phase Volume gets resorbed Volume over-load may occur This is the phase where people die because of the problems faced during the critical stage
IgG antibody - specific to the initial infecting DV serotype + cross reacting antibody IgM antibody to the secondary infecting DV serotype Following primary infection – Specific antibody response + CMI (memory T cells) Cross reactive antibody response + CMI (memory T cells) Dr. S Guanasena
Investigations • CBC and platelet count • First 5 days • NS 1 • PCR • >5 days • IgM • IgG
Update on vaccine • Chimera vaccine • Yellow fever & dengue • Launched 2016 • Partial immunity • Risk of secondary infection • Attenuated vaccine • 6-8 cycles in DKC (Dog kidney cells)
HAVE WE DONE ENOUGH? Asia pacific strategic plan for control of Dengue (2010-2015) What are our Goals????? • Decrease prevalence by 10% per year • Keep DHF mortality below 1%
Current situation in Punjab Lahore2011 Rawalpindi2015 DEN 1,2,3,4 2349 cases (uptill 27-10-2015) > 300 cases of DHF and DSS 10 deaths • DEN 2 • Innumerable • Few DHF DEAG TRINED MEDICS AND PARAMEDICS = 13000
Current situation in Punjab Lahore, 2016 Rawalpindi, 2016 DEN 1,2,3 299 18 03 deaths • DEN 1 • 109 • Few DHF • No death DEAG TRINED MEDICS AND PARAMEDICS = 3165
Take Home message We can prevent quite a few deaths ---- if we can Differentiate DF from DHF Diagnose the onset of critical phase (phase of leaking) Give appropriate fluids