Download
1 / 24
240 likes | 270 Vues
How can we possibly get smoking prevalence below 20%. Robert West University College London www.rjwest.co.uk. Outline. Current trends in smoking Principles underpinning policy options Analysis of future policy options Recommendations. Smoking prevalence in the UK. 25%. GHS 2005.

E N D
How can we possibly get smoking prevalence below 20% Robert West University College London www.rjwest.co.uk
Outline • Current trends in smoking • Principles underpinning policy options • Analysis of future policy options • Recommendations
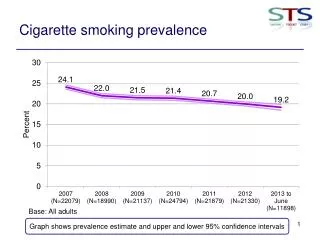
Smoking prevalence in the UK 25% GHS 2005
Numbers of smokers in the UK www.rjwest.co.uk
Smoking mortality in the UK • Mortality attributable to smoking has declined sharply over the past 10 years: 131,000 in 1995 to an estimated 93,000 in 2005; 28,000 under 70 years • The decline is largely due to the steep decline in smoking prevalence that took place 10-20 years ago • In 2020 the death rate is estimated at approximately 66,000; 18,000 under 70 www.rjwest.co.uk
What underlies the reduction in prevalence? • ONS annual surveys (October/November) • 4% prevalence reduction in 10 years • Appears to be attributable to increase in ‘never-smokers’ • But quit ratio (ex-smokers as a proportion of ever-smokers) has increased slightly • So decreased uptake historically and increased current cessation probably play a role Taylor et al, ONS 2006
Trends in motivation to quit • ONS annual surveys • no evidence for change in desire or intention to quit • desire to quit among manual occupational groups equals that of professionals • possibly greater intention to quit in professionals Taylor et al, ONS 2006
Smoking Impulse to smoke Cues/triggers Anticipated enjoyment Desire to smoke Need to smoke Nicotine ‘hunger’ Unpleasant mood and physical symptoms Anticipated benefit Reminders Positive evaluations of smoking Smoker ‘identity’ Beliefs about benefits of smoking Principles underpinning policy 1: Motivation to smoke www.primetheory.com
Not smoking Inhibition Cues/triggers Anticipated praise Desire not to smoke Need not to smoke Plan not to smoke Anticipated disgust, guilt or shame Fears about health Anticipated self-respect Reminders Positive evaluations of not smoking Non-smoker ‘identity’ Beliefs about benefits of not smoking Principles underpinning policy 2: Motivation not to smoke www.primetheory.com
Principles underlying policy options 3: Economic concepts • Financial incentives • Concept: Increase the financial cost relative to ability to pay • Barriers: Social and political resistance, lower affordability of other goods, possible substitution for other incentives, get-arounds • Moral and social incentives • Concept: Increase the feeling of moral and normative pressure • Barriers: Difficult to achieve, risk of backlash, stigmatisation of those that do not change • Personal incentives • Concept: Change balance of perceived personal happiness/ease and discomfort/effort in favour of not smoking • Barriers: Practical and financial constraints may limit reach and effectiveness
Principles underpinning policy 3: Health promotion concepts West, R British Medical Bulletin, In Press
Future policy options • Price increases • increase taxes • reduce options for cheap smoking • Smoke-free legislation • Increasing access to help with stopping • Mass media campaigns and media advocacy • Warning labels on tobacco packaging • Further work on restricting tobacco promotion • Decreasing youth access to tobacco • School-based programmes See Framework Convention on Tobacco Control; Levy et al (2004) Journal of Public Health Management and Practice, 10, 338-353; West, R British Medical Bulletin, In Press
In reverse order of likely future benefit ... • School-based programmes • Little evidence that stepping up school campaigns would have an effect • Decreasing youth access to tobacco • Little to suggest that raising the age of purchasing will have an impact, though it could if sanctions on vendors were increased and ID cards required • Further work on tobacco promotion • Not clear what further can be done but need to tackle any attempts by tobacco industry to circumvent • Warning labels on tobacco packaging • Indirect evidence (e.g. on awareness and attitudes) of effects of pictorial warnings but effect size difficult to quantify • Mass media campaigns and media advocacy • Possible to show immediate increases in markers of quitting such as NRT sales effects following media campaigns and No Smoking Day • Substantial stepping up well-crafted campaigns likely to have an effect but the size cannot be quantified
3. Increasing access to treatment • Current access to treatment to aid cessation • Prescription and OTC medication (e.g. NRT): With 30% using it each year and a 5% effect size it may be prevalencing by about 0.4% • NHS stop smoking services: With 5% using them each year and an added benefit over medication of 5% they may be reducing prevalence by about 0.06% each year • Total current effect: 0.46% per year • Potential for the future • Increasing medication usage to 40% and NHS service usage to 8% could reduce prevalence by a further 0.16% per year
2. Smoke-free legislation • Effect on prevalence is difficult to gauge because of limited relevant international comparisons • Ireland: Reduction of up to 2% in prevalence, but from a higher prevalence base • Effect in the England is difficult to quantify because it is starting from a more smoke-free initial position but 0.5% -1% is possible
1. Price increases • By common consensus the intervention most likely to reduce prevalence significantly is an increase in price • In the UK, non-duty paid tobacco and cigarettes represent a major part of the market so the two key measures are: • Reducing access to cheap smoking • Increasing the duty on cigarettes and rolling tobacco
Reducing smuggling • 25% of cigarettes and 75% of hand-rolled tobacco smoked have avoided UK taxes • Legal cross border traffic in cigarettes account for 8-10% of the cigarette market • Hand-rolled cigarettes is particularly common among the unemployed • The average price of 20 illicit cigarettes is about half that of licit cigarettes (£2.50 versus £4.89) • In theory eliminating ‘cheap smoking’ could raise the average cost of smoking by 20% which could decrease prevalence by 2% to 4% • The problem is that it is expensive and difficult to implement effective measures See ASH Factsheet 17 (www.ash.org.uk) Chief Medical Officer report 2004
Tax increases • Consumption elasticity in western countries is approximately 40%; ‘participation’ elasticity (numbers of smokers) appears to account for most though not all of this • Therefore, other things being equal, a 20p (4%) increase in cost of cigarettes through taxation would decrease prevalence by between .5 and 1% even if it only affected the taxed tobacco market • This would cut the number of smokers by at least 240,000 and ultimately save an estimated 100,000 lives • The price would then have to be kept at least in line with earnings to avoid back-sliding
The Californian experience • Proposition 99 put the price up and devoted 5 cents per pack to tobacco control • An immediate effect on prevalence but then a flattening off
The French experience • France recently put the price of cigarettes up by 40% • The effect was an ~ 25% immediate reduction in consumption and transient increases in use of cessation aids • This was despite the ease of cross-border trafficking http://www.ofdt.fr/ofdtdev/live/donneesnat/tabtabac.html
Some information on price rises • The effect is greatest in: • low income smokers • adolescent smokers • pregnant smokers • Cigarettes are more ‘affordable’ now than in the 1960s (Guindon et al: Tob Control. 2002, 11:35-43) • In those who do not smoke, consumption elasticity will reduce the cost • The main threat is an increased move to ‘cheap smoking’ See West, R British Medical Bulletin, In Press for a review
Putting it all together • On current projections it is doubtful that we will reach 21% in 2010 but in any event we must set our sights on getting well below 20% • We need something to kick-start the next major downward movement in prevalence • Increasing the duty on cigarettes by 20p over and above rises in line with earnings will have an immediate effect • Putting ALL the funds generated (£350-£400 million per year) into a Tobacco Control Task Force would provide a stable source of funding to enable: • more effective anti-smuggling operations which should more than pay for themselves and ultimately be a ‘no-cost measure’ • a substantial and sustained increase in mass media campaigns • a policy and legal team of sufficient size to work effectively on all the fronts necessary to mount a comprehensive, sustained tobacco control programme in the spirit of the FCTC • The Treasury has until now baulked at ‘hypothecation’ but has now accepted it for education spending
Public support? • UK arm (N=700) of a pan-European survey European Survey on Tobacco Control Attitudes and Knowledge (ESTA) • a population-based, representative survey of n=3.500 participants age 16-59, in 5 different European countries (Germany, Greece, Poland, Sweden, UK) • Conducted between January and April 2006 • Preliminary evidence suggests that there would be public support for such a measure • The population appears to be generally in favour of using taxation to control smoking
Conclusions • The UK tobacco control programme has many strong points ... • smoke-free public and work places • a ban on tobacco advertising • excellent access to effective help with stopping • well-designed mass media campaigns • ... but progress in reducing prevalence is painfully slow • To start the next major downward shift we need to kick-start the process with a modest real-terms price increase (20p) and use the funds exclusively to run a Tobacco Control Task Force to step up the other measures that will have an impact saving hundreds of thousands of lives • There is preliminary evidence that the public would support this