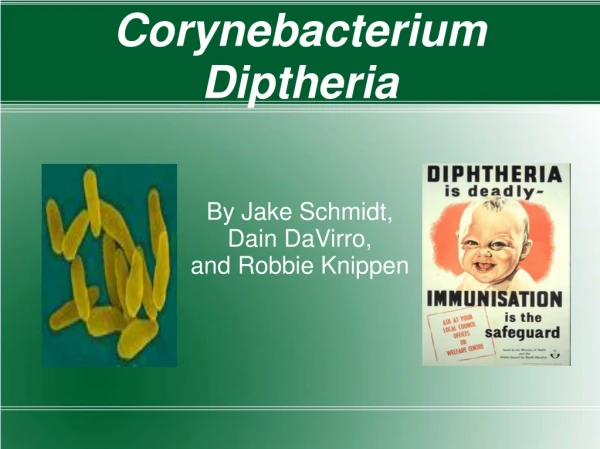
Corynebacterium diphtheriae
Corynebacterium diphtheriae. methylene blue stain. Albert stain. metachromatic granules. Morphology.

Corynebacterium diphtheriae
E N D
Presentation Transcript
methylene blue stain Albert stain metachromatic granules Morphology • Another characteristic is the presence of metachromatic granules (RNA and polymetaphosphate) in bacterial cells. The granules are bluish-purple with methylene blue, and dark purple by Albert staining method.
Culture • Aerobic and facultative anaerobic, growing well at 37C on blood- or serum-containing medium. • Loeffler’s serum slant: not a selective medium but gives abundant growth and typical morphology of the bacillus. • Blood tellurite agar: a selective medium because tellurite can suppress the growth of normal flora in throat, and the colonies are black-colored.
Pediatric • Symptoms: • formation of a false membrane in the throat • high fever • difficulty in breathing
Diphtheriais a typical toxigenic infectious disease. Diphtheria toxin is the major virulent factor. • Effective antitoxin therapy and successful toxoid vaccine available. • A rare disease, still occur in non-immunized populations. • High death rate.
Virulent factor: diphtheria toxin • The toxin encoding gene (tox) is carried byβ-corynebacteriophage • only the bacillus infected by the phage and committed lysogenic conversion produce diphtheria toxin • The regulation of tox gene expression is mediated by an iron-activated inhibitor (DtxR) which is chromosomally encoded by C. diphtheria
Cell surface Toxic Binding A B ◆many exotoxins are called as A-B type toxins because they consist of A and B subunits. The B subunit generally mediates the toxin complex molecule to adhere and then enter the host cell. A subunit provides the toxic activity.
Diphtheria toxin is an A-B type toxin • A diphtheria toxin molecule contains 535 amino acids with subunit A and subunit B. • Subunit B contains receptor binding and transmembrane domains. • Subunit A contains catalytic domain. It inactivate elongation factor 2 (EF2). Thus the protein synthesis is suppressed.
The toxin is very toxic to humans and many animals (e.g.,monkey, rabbit, guinea-pig). • Particularly harmful to heart and central nervous system. • The lethal dose is as low as 100 to 150 ng/kg.
Clinical Manifestations • Corynebacterium diphtheriae can cause pharyngitis which leads to formation of thick grey membrane called pseudo-membrane. The pseudo-membrane is composed of fibrin, dead epithelial cells, bacteria and neutrophils. It exfoliates easily and then blocks the airway which results in hypoxia (缺氧) and suffocation (窒息). • As a result of the action of diphtheria toxin to peripheral motor neurons and myocardium, life-threatening systemic complications (principally loss of motor function and congestive heart failure) may develop.
Diagnosis of diphtheria requires laboratory confirmation of toxigenic Corynebacterium diphtheriae. • It is usually determined by in vitro tests such as Elek immunodiffusion test.
Diphtheria patients must be promptly treated with antitoxin to neutralize circulating (free) diphtheria toxin. Antitoxin cannot neutralize the toxicity of exotoxin that has bound to the host cells. • Antibiotics (penicillin and erythromycin) are used as part of the treatment. • Diphtheria toxoid is a component of the DPT vaccine, which includes diphtheria toxoid, killed whole cell pertussis(Bordetella pertussis)and tetanus toxoid(Clostridium tetani).
Acid-fast bacilli Mycobacteria do not stain readily. However, if these bacteria are once stained by Ziel-Neelsen Acid-Fast Stain method, they are able to resist decolorization by acid or alcohol.
Amongthe species ofMycobacteria, M. tuberculosis is the most important pathogen that causes human tuberculosis. • M. bovis is a zoonotic causative agent of cattle tuberculosis. It also causes human tuberculosis. • M. leprae is the causative agent of leprosy which is still present in the third world.
Morphology and culture • Mycobacterium tuberculosis hasthe typical morphology and acid-fast property of Mycobacteria. • Lowenstein-Jensen medium is the widely used medium for cultivating Mycobacterium tuberculosis. In this medium, malachite green (孔雀绿) is included to inhibit other bacteria. • The growth rate is slower than most other bacteria. The doubling time is about 18 hours.
The colonies are formed after 3-6 weeks of incubation on Lowenstein-Jensen medium. The colonies are buff colored and dry breadcrumb-like.
Variation • Drug resistance variation: Many clinical isolates of Mycobacterium tuberculosis are drug-resistant. • Virulence variation: BCG (Bacillus Calmette-Guerin) is the human tuberculosis vaccine. It is a preparation of live attenuated Mycobacterium bovis. • L-form: a form that lacks the cell wall
Virulent factors • Produce no endotoxin, exotoxin or invasive enzymes • The pathogenicity is due to cell wall components, and substances inducing immunopathological reactions.
Virulent factors Lipids in the cell wall • Cord factor: lipoarabinomannan, damages mitochondria • Phosphatide: causes the formation of tubercule and granuloma • Sulfatides: inhibits phagosome-lysosome fusion • Wax D: serves as an “adjuvant” that induce hypersensitive reaction.
Virulent factors • Proteins • e.g., Tuberculin mixed with wax D can induce hypersensitive reaction. • Polysaccharide • Bound to wax D to induce the infiltration (浸润) of inflammatory cells.
Tissue destruction results from cell-mediated hypersensitivity. Pathogenesis Mycobacterium tuberculosisenters alveoli by airborne transmission It resists destruction by alveolar macrophages and propagate To cause primary tuberculosis To spread to lymph nodes Cell-mediated immune response stops cycle of destruction and spread. To enter bloodstream and seed other organs To reseed the lungs To lead to post-primary tuberculosis
Mycobacteriumtuberculosisis transmitted through droplet and airborne dust containing the microbe. • Mycobacteriumtuberculosishas multiple routes invading human body, such as respiratory tract, intestinal tract and skin, to cause various tuberculosis. • Among the different tuberculosis, pulmonary tuberculosis is the most common form. Transmission and infection
Bacteriological examination: the definitive diagnosis for tuberculosis based on the presence of acid-fast bacteria in the sputum (pulmonary tuberculosis) and in other clinical samples. • Tuberculin skin test: is a method of identifying persons who once infected with Mycobacterium tuberculosis.
Tuberculin skin testis performed by an intradermal injection of 5 tuberculin units / 0.1 ml of purified protein derivative (PPD) into forearm. The result (diameter of induration around the site of injection) is read 48 to 72 hours after the injection. • A tuberculin reaction of >= 5 mm of induration is classified as positive result. However, a positive test only means to exposure once to the microorganism but does not certainly indicate active disease.
Prevention:Vaccination of BCG vaccine. • Treatment: Antibiotics used to treat tuberculosissuch as streptomycin, isoniazid, rifampin etc., are quite different from those used to treat other bacterial infectious diseases. Clinically, several anti-tuberculosis drugs must be simultaneously applied to avoid drug resistance and to increase efficiency of therapy.